

Trends in U.S. Extracorporeal Membrane Oxygenation Use and Outcomes: 2002-2012
- PMID: 26686427
- PMCID: PMC4780346
- DOI: 10.1053/j.semtcvs.2015.07.005
Trends in U.S. Extracorporeal Membrane Oxygenation Use and Outcomes: 2002-2012
Abstract
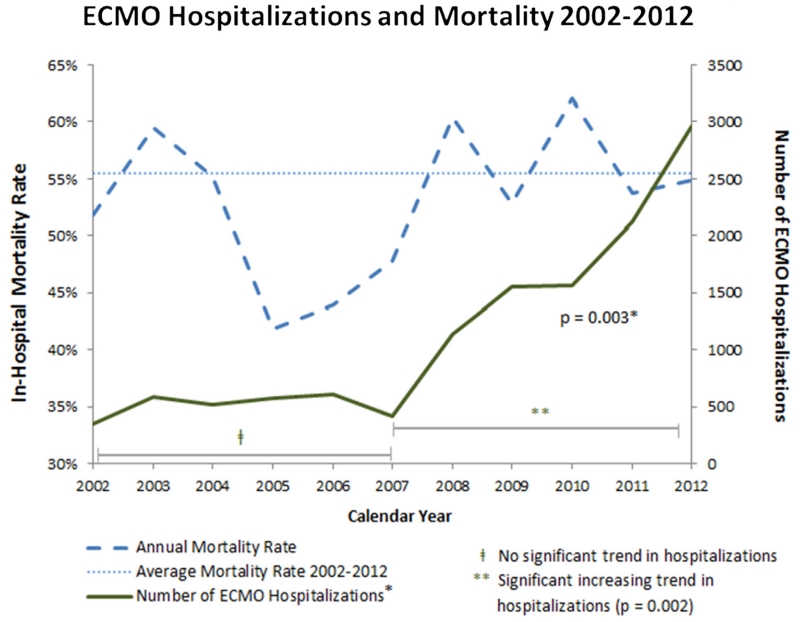
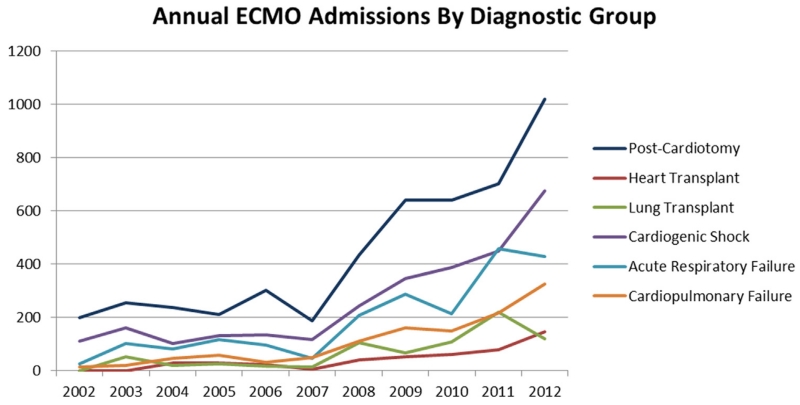
This study evaluates contemporary trends in the use and outcomes of adult patients undergoing extracorporeal membrane oxygenation (ECMO) in U.S. hospitals. All adult discharges in the Nationwide Inpatient Sample database during the years 2002-2012 that included ECMO were used to estimate the total number of U.S. ECMO hospitalizations (n = 12,407). Diagnostic codes were used to group patients by indication for ECMO use into postcardiotomy, heart transplant, lung transplant, cardiogenic shock, respiratory failure, and cardiopulmonary failure. A Mann-Kendall test was used to examine trends over time using standard statistical techniques for survey data. We found that ECMO use increased significantly from 2002-2012 (P = 0.003), whereas in-hospital mortality rate fluctuated without a significant difference in trend over time. No significant trend was observed in overall ECMO use from 2002-2007, but the use did demonstrate a statistically significant increase from 2007-2012 (P = 0.0028). The highest in-hospital mortality rates were found in the postcardiotomy (57.2%) and respiratory failure (59.2%) groups. Lung and heart transplant groups had the lowest in-hospital mortality rates (44.10% and 45.31%, respectively). The proportion of ECMO use for postcardiotomy decreased from 56.9% in 2002 to 37.9% in 2012 (P = 0.026) and increased for cardiopulmonary failure from 3.9% to 11.1% (P = 0.026). We concluded that ECMO use in the United States increased between 2002 and 2012, driven primarily by increase in national ECMO use beginning in 2007. Mortality rates remained high but stable during this time period. Though there were shifts in relative ECMO use among patient groups, absolute ECMO use increased for all indications over the study period.
Copyright © 2015. Published by Elsevier Inc.
Figures
Comment in
-
It is Worth it to Increase the Use of Extracorporeal Membrane Oxygenation?Semin Thorac Cardiovasc Surg. 2015 Summer;27(2):89-90. doi: 10.1053/j.semtcvs.2015.09.001. Epub 2015 Oct 5. Semin Thorac Cardiovasc Surg. 2015. PMID: 26686428 No abstract available.
References
-
- Zapol WM, Snider MT, Hill J, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure: A randomized prospective study. J Am Med Assoc. 1979;242(20):2193–2196. - PubMed
-
- Karamlou T, Vafaeezadeh M, Parrish AM, et al. Increased extracorporeal membrane oxygenation center case volume is associated with improved extracorporeal membrane oxygenation survival among pediatric patients. J Thorac Cardiovasc Surg. 2013;145(2):470–475. - PubMed
-
- Paden ML, Rycus PT, Thiagarajan RR, et al. Update and outcomes in extracorporeal life support. Semin Perinatol. 2014;38(2):65–70. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
