

Patient-reported outcomes with anastrozole versus tamoxifen for postmenopausal patients with ductal carcinoma in situ treated with lumpectomy plus radiotherapy (NSABP B-35): a randomised, double-blind, phase 3 clinical trial
- PMID: 26686960
- PMCID: PMC4792658
- DOI: 10.1016/S0140-6736(15)01169-1
Patient-reported outcomes with anastrozole versus tamoxifen for postmenopausal patients with ductal carcinoma in situ treated with lumpectomy plus radiotherapy (NSABP B-35): a randomised, double-blind, phase 3 clinical trial
Abstract
Background: The NSABP B-35 trial compared 5 years of treatment with anastrozole versus tamoxifen for reducing subsequent occurrence of breast cancer in postmenopausal patients with ductal carcinoma in situ. This report assesses the effect of these drugs on quality of life and symptoms.
Methods: The study was done at 333 hospitals in North America. Postmenopausal women with hormone-positive ductal carcinoma in situ treated by lumpectomy with clear resection margins and whole breast irradiation were randomly assigned to receive either tamoxifen (20 mg/day) or anastrazole (1 mg/day) for 5 years, stratified by age (<60 years vs ≥60 years). Patients and investigators were masked to treatment allocation. Patients completed questionnaires at baseline and every 6 months thereafter for 6 years. The primary outcomes were SF-12 physical and mental health component scale scores, and vasomotor symptoms (as per the BCPT symptom scale). Secondary outcomes were vaginal symptoms and sexual functioning. Exploratory outcomes were musculoskeletal pain, bladder symptoms, gynaecological symptoms, cognitive symptoms, weight problems, vitality, and depression. We did the analyses by intention to treat, including patients who completed questionnaires at baseline and at least once during follow-up. This study is registered with ClinicalTrials.gov, NCT00053898.
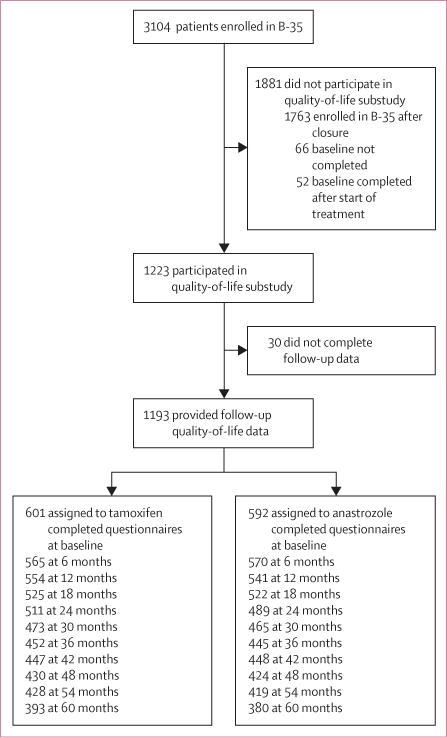
Findings: Between Jan 6, 2003, and June 15, 2006, 3104 patients were enrolled in the study, of whom 1193 were included in the quality-of-life substudy: 601 assigned to tamoxifen and 592 assigned to anastrozole. We detected no significant difference between treatment groups for: physical health scores (mean severity score 46·72 for tamoxifen vs 45·85 for anastrozole; p=0·20), mental health scores (52·38 vs 51·48; p=0·38), energy and fatigue (58·34 vs 57·54; p=0·86), or symptoms of depression (6·19 vs 6·39; p=0·46) over 5 years. Vasomotor symptoms (1·33 vs 1·17; p=0·011), difficulty with bladder control (0·96 vs 0·80; p=0·0002), and gynaecological symptoms (0·29 vs 0·18; p<0·0001) were significantly more severe in the tamoxifen group than in the anastrozole group. Musculoskeletal pain (1·50 vs 1·72; p=0·0006) and vaginal symptoms (0·76 vs 0·86; p=0·035) were significantly worse in the anastrozole group than in the tamoxifen group. Sexual functioning did not differ significantly between the two treatments (43·65 vs 45·29; p=0·56). Younger age was significantly associated with more severe vasomotor symptoms (mean severity score 1·45 for age <60 years vs 0·65 for age ≥60 years; p=0·0006), vaginal symptoms (0·98 vs 0·65; p<0·0001), weight problems (1·32 vs 1·02; p<0·0001), and gynaecological symptoms (0·26 vs 0·22; p=0·014).
Interpretation: Given the similar efficacy of tamoxifen and anastrozole for women older than age 60 years, decisions about treatment should be informed by the risk for serious adverse health effects and the symptoms associated with each drug. For women younger than 60 years old, treatment decisions might be driven by efficacy (favouring anastrozole); however, if the side-effects of anastrozole are intolerable, then switching to tamoxifen is a good alternative.
Funding: US National Cancer Institute, AstraZeneca Pharmaceuticals.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
MEC has received research support from Novartis, fees from Biotheranostics for participation on an advisory board, and fees from Roche and Abbvie. All other authors declare no competing interests.
Figures



Comment in
-
Endocrine treatment for ductal carcinoma in situ: balancing risks and benefits.Lancet. 2016 Feb 27;387(10021):819-21. doi: 10.1016/S0140-6736(15)01219-2. Epub 2015 Dec 11. Lancet. 2016. PMID: 26686312 No abstract available.
References
-
- American Cancer Society. Breast Cancer Facts and Figures 2015–2016. Atlanta: American Cancer Society; 2015.
-
- Fisher B, Costantino J, Redmond C, et al. Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med. 1993;328:1581–86. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16:441–52. - PubMed
-
- Fisher B, Land S, Mamounas E, Dignam J, Fisher ER, Wolmark N. Prevention of invasive breast cancer in women with ductal carcinoma in situ: an update of the National Surgical Adjuvant Breast and Bowel Project experience. Semin Oncol. 2001;28:400–18. - PubMed
-
- Fisher B, Dignam J, Wolmark N, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353:1993–2000. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
