

Differential Effects of β-Blockers, Angiotensin II Receptor Blockers, and a Novel AT2R Agonist NP-6A4 on Stress Response of Nutrient-Starved Cardiovascular Cells
- PMID: 26691397
- PMCID: PMC4686716
- DOI: 10.1371/journal.pone.0144824
Differential Effects of β-Blockers, Angiotensin II Receptor Blockers, and a Novel AT2R Agonist NP-6A4 on Stress Response of Nutrient-Starved Cardiovascular Cells
Abstract
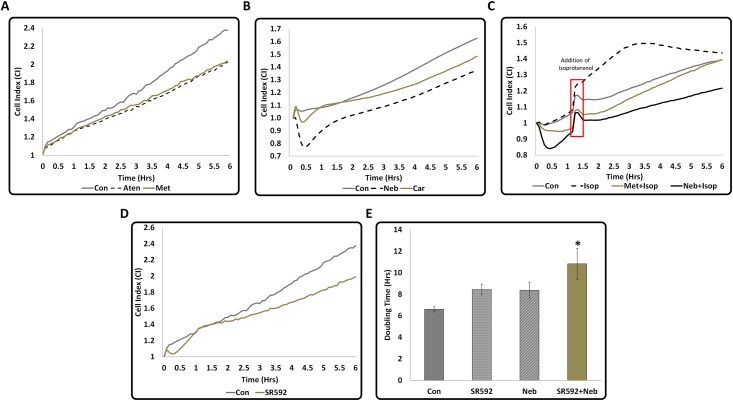
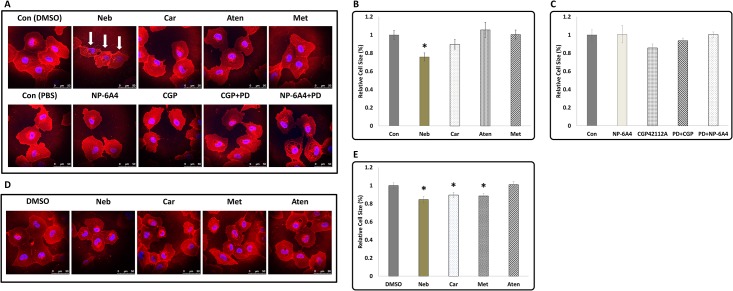
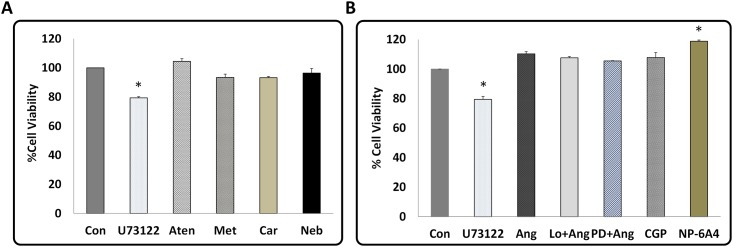
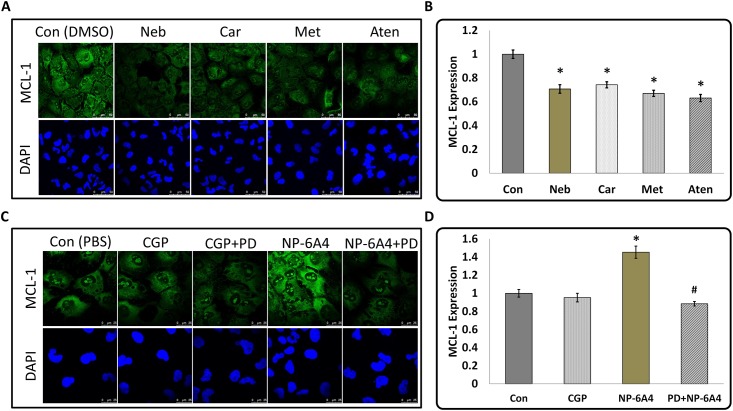
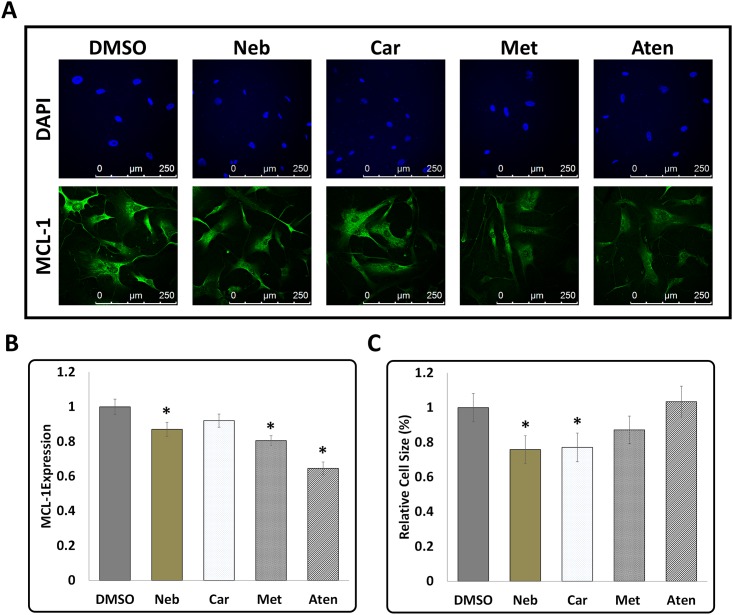
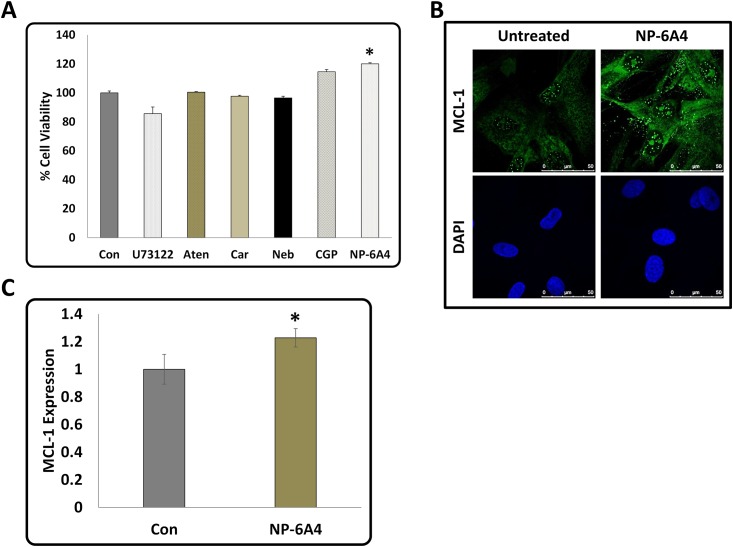
In order to determine differences in cardiovascular cell response during nutrient stress to different cardiovascular protective drugs, we investigated cell responses of serum starved mouse cardiomyocyte HL-1 cells and primary cultures of human coronary artery vascular smooth muscles (hCAVSMCs) to treatment with β-blockers (atenolol, metoprolol, carvedilol, nebivolol, 3 μM each), AT1R blocker losartan (1 μM) and AT2R agonists (CGP42112A and novel agonist NP-6A4, 300 nM each). Treatment with nebivolol, carvedilol, metoprolol and atenolol suppressed Cell Index (CI) of serum-starved HL-1 cells (≤17%, ≤8%, ≤15% and ≤15% respectively) as measured by the Xcelligence Real-Time Cell Analyzer (RTCA). Conversely, CI was increased by Ang II (≥9.6%), CGP42112A (≥14%), and NP-6A4 (≥25%) respectively and this effect was blocked by AT2R antagonist PD123319, but not by AT1R antagonist losartan. Thus, the CI signature for each drug could be unique. MTS cell proliferation assay showed that NP-6A4, but not other drugs, increased viability (≥20%) of HL-1 and hCAVSMCs. Wheat Germ Agglutinin (WGA) staining showed that nebivolol was most effective in reducing cell sizes of HL-1 and hCAVSMCs. Myeloid Cell Leukemia 1 (MCL-1) is a protein critical for cardiovascular cell survival and implicated in cell adhesion. β-blockers significantly suppressed and NP-6A4 increased MCL-1 expression in HL-1 and hCAVSMCs as determined by immunofluorescence. Thus, reduction in cell size and/or MCL-1 expression might underlie β-blocker-induced reduction in CI of HL-1. Conversely, increase in cell viability and MCL-1 expression by NP-6A4 through AT2R could have resulted in NP-6A4 mediated increase in CI of HL-1. These data show for the first time that activation of the AT2R-MCL-1 axis by NP-6A4 in nutrient-stressed mouse and human cardiovascular cells (mouse HL-1 cells and primary cultures of hCAVSMCs) might underlie improved survival of cells treated by NP-6A4 compared to other drugs tested in this study.
Conflict of interest statement
Figures

Similar articles
-
AT2R agonist NP-6A4 mitigates aortic stiffness and proteolytic activity in mouse model of aneurysm.J Cell Mol Med. 2020 Jul;24(13):7393-7404. doi: 10.1111/jcmm.15342. Epub 2020 May 18. J Cell Mol Med. 2020. PMID: 32420690 Free PMC article.
-
Cell-Specific Protective Signaling Induced by the Novel AT2R-Agonist NP-6A4 on Human Endothelial and Smooth Muscle Cells.Front Pharmacol. 2018 Aug 21;9:928. doi: 10.3389/fphar.2018.00928. eCollection 2018. Front Pharmacol. 2018. PMID: 30186168 Free PMC article.
-
Suppression of Inflammatory Cardiac Cytokine Network in Rats with Untreated Obesity and Pre-Diabetes by AT2 Receptor Agonist NP-6A4.Front Pharmacol. 2021 Jun 18;12:693167. doi: 10.3389/fphar.2021.693167. eCollection 2021. Front Pharmacol. 2021. PMID: 34220518 Free PMC article.
-
AT2 receptor activities and pathophysiological implications.J Cardiovasc Pharmacol. 2015 Mar;65(3):226-32. doi: 10.1097/FJC.0000000000000208. J Cardiovasc Pharmacol. 2015. PMID: 25636068 Free PMC article. Review.
-
β-blockers: a review of their pharmacological and physiological diversity in hypertension.Ann Pharmacother. 2014 Jun;48(6):723-33. doi: 10.1177/1060028013519591. Epub 2014 Mar 31. Ann Pharmacother. 2014. PMID: 24687542 Review.
Cited by
-
Anti-fibrotic Potential of AT2 Receptor Agonists.Front Pharmacol. 2017 Aug 31;8:564. doi: 10.3389/fphar.2017.00564. eCollection 2017. Front Pharmacol. 2017. PMID: 28912715 Free PMC article. Review.
-
Protection of Sacubitril/Valsartan against Pathological Cardiac Remodeling by Inhibiting the NLRP3 Inflammasome after Relief of Pressure Overload in Mice.Cardiovasc Drugs Ther. 2020 Oct;34(5):629-640. doi: 10.1007/s10557-020-06995-x. Cardiovasc Drugs Ther. 2020. PMID: 32444995 Free PMC article.
-
Molecular docking, 3D-QSAR and structural optimization on imidazo-pyridine derivatives dually targeting AT1 and PPARg.Oncotarget. 2017 Apr 11;8(15):25612-25627. doi: 10.18632/oncotarget.15778. Oncotarget. 2017. PMID: 28445965 Free PMC article.
-
AT2R agonist NP-6A4 mitigates aortic stiffness and proteolytic activity in mouse model of aneurysm.J Cell Mol Med. 2020 Jul;24(13):7393-7404. doi: 10.1111/jcmm.15342. Epub 2020 May 18. J Cell Mol Med. 2020. PMID: 32420690 Free PMC article.
-
Regulation of the cardioprotective adiponectin and its receptor AdipoR1 by salt.Can J Physiol Pharmacol. 2017 Mar;95(3):305-309. doi: 10.1139/cjpp-2016-0570. Epub 2016 Nov 30. Can J Physiol Pharmacol. 2017. PMID: 28051329 Free PMC article.
References
-
- World health Organization (2014). The top 10 causes of death. http://www.who.int/mediacentre/factsheets/fs310/en/
-
- Center for Disease Control and Prevention Fact Sheets (Feb 6th 2015). Leading Causes of Death. http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
