

Performance of magnetic resonance elastography in primary sclerosing cholangitis
- PMID: 26691631
- PMCID: PMC4885758
- DOI: 10.1111/jgh.13263
Performance of magnetic resonance elastography in primary sclerosing cholangitis
Abstract
Background and aim: Liver stiffness (LS) measured by magnetic resonance elastography (MRE) is emerging as an important biomarker in chronic liver diseases. We examined the diagnostic performance of MRE, factors associated with an increased LS and the prognostic value of LS as measured by MRE among patients with primary sclerosing cholangitis (PSC).
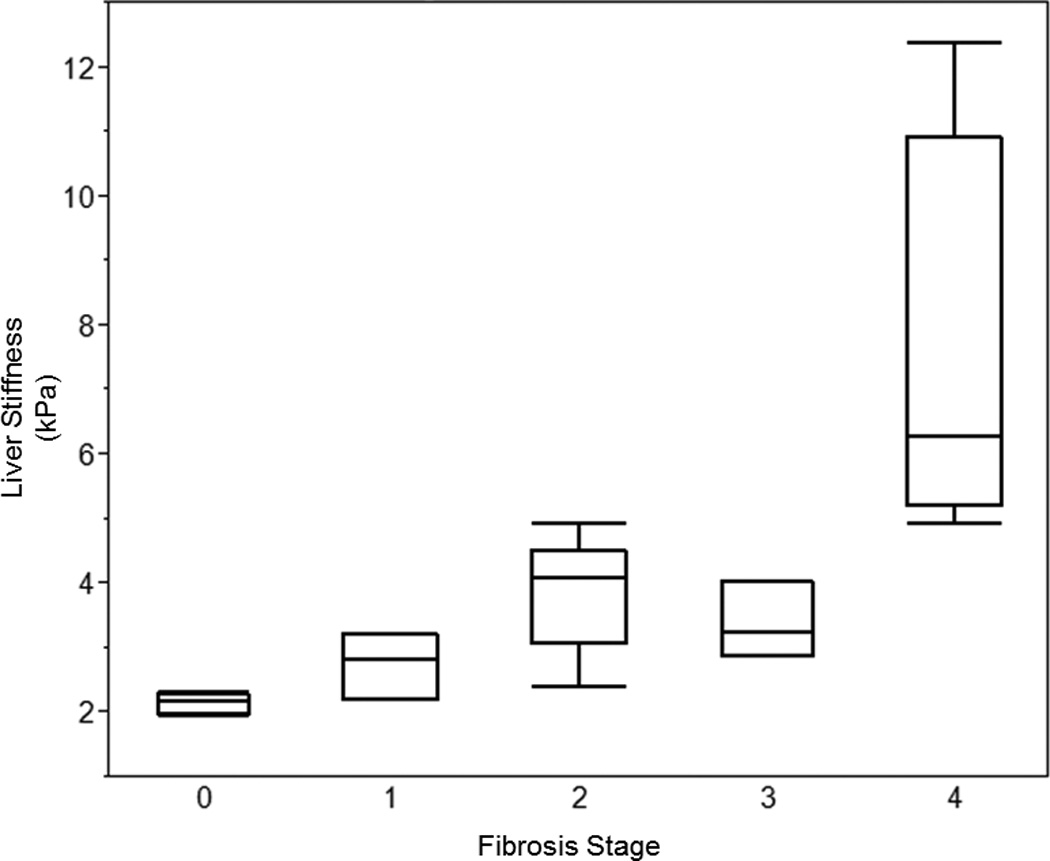
Methods: We performed a retrospective review of 266 patients with PSC to examine whether LS was associated with the primary endpoint of hepatic decompensation (ascites, variceal hemorrhage and hepatic encephalopathy). The ability of MRE to differentiate stages of fibrosis was examined in a subset of patients who underwent a liver biopsy (n = 20).
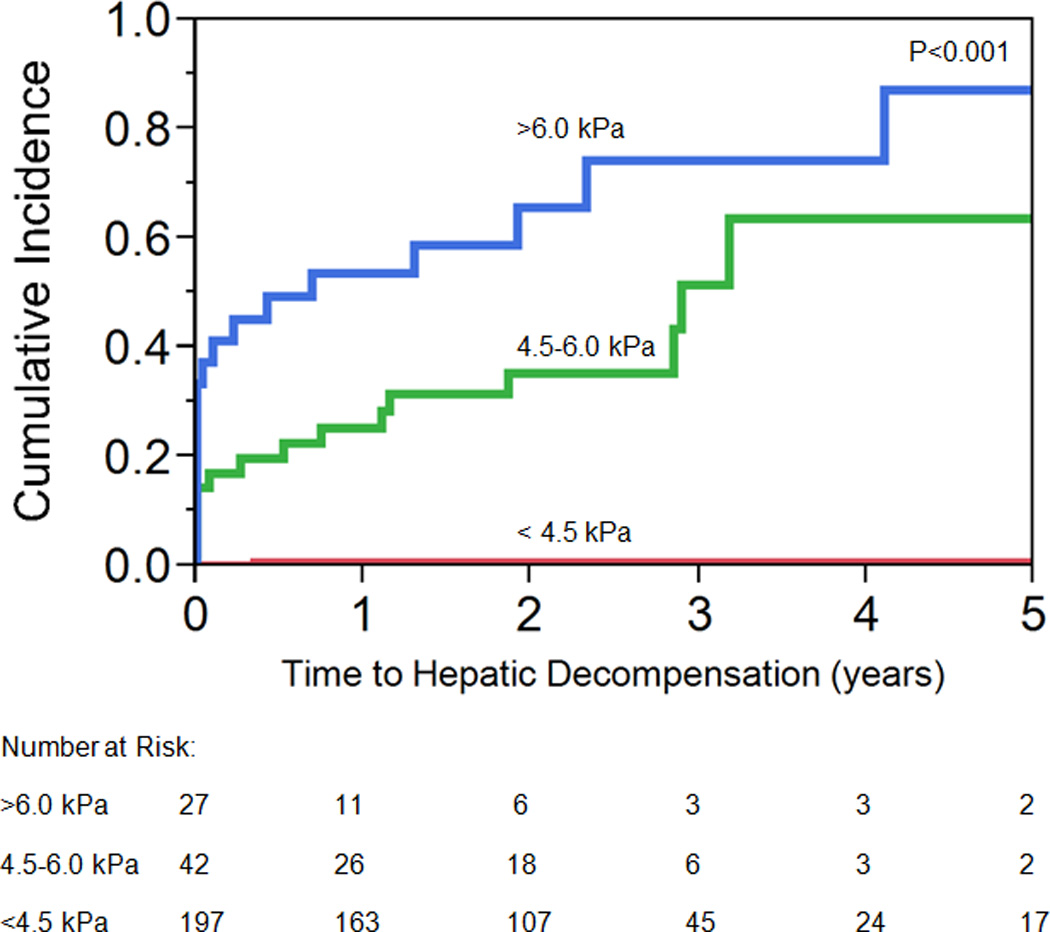
Results: An LS of 4.93 kPa was the optimal point to detected F4 fibrosis (sensitivity, 1.00; 95% confidence interval (CI), 0.40-1.00; specificity, 0.94; 95%CI, 0.68-1.00). While a serum alkaline phosphatase <1.5 times the upper limit of normal excluded the presence of advanced LS, it was not associated with the primary endpoint (hazard ratio, 0.26; 95%CI, 0.01-1.33). However, LS was associated with the development of decompensated liver disease (hazard ratio, 1.55; 95%CI, 1.41-1.70). The optimal LS thresholds that stratified patients at a low, medium and high risk for hepatic decompensation were <4.5, 4.5-6.0 and >6.0 kPa (respectively).
Conclusion: Magnetic resonance elastography is able to detect cirrhosis with high specificity and an alkaline phosphatase <1.5 times the upper limit of normal makes the presence of advanced LS unlikely. Moreover, LS obtained by MRE is predictive of hepatic decompensation in PSC.
Keywords: liver stiffness; magnetic resonance elastography; primary sclerosing cholangitis.
© 2015 Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
Conflicts of Interests & Disclosure Statement: The remaining coauthors have nothing else to disclose.
Figures
Similar articles
-
Changes in Liver Stiffness, Measured by Magnetic Resonance Elastography, Associated With Hepatic Decompensation in Patients With Primary Sclerosing Cholangitis.Clin Gastroenterol Hepatol. 2020 Jun;18(7):1576-1583.e1. doi: 10.1016/j.cgh.2019.10.041. Epub 2019 Nov 1. Clin Gastroenterol Hepatol. 2020. PMID: 31683058 Free PMC article.
-
The development and validation of magnetic resonance elastography for fibrosis staging in primary sclerosing cholangitis.Eur Radiol. 2019 Feb;29(2):1039-1047. doi: 10.1007/s00330-018-5619-4. Epub 2018 Jul 26. Eur Radiol. 2019. PMID: 30051141
-
Baseline values and changes in liver stiffness measured by transient elastography are associated with severity of fibrosis and outcomes of patients with primary sclerosing cholangitis.Gastroenterology. 2014 Apr;146(4):970-9; quiz e15-6. doi: 10.1053/j.gastro.2013.12.030. Epub 2013 Dec 31. Gastroenterology. 2014. PMID: 24389304
-
Role of spleen elastography in patients with chronic liver diseases.World J Gastroenterol. 2016 Sep 21;22(35):7857-67. doi: 10.3748/wjg.v22.i35.7857. World J Gastroenterol. 2016. PMID: 27672283 Free PMC article. Review.
-
MR elastography in primary sclerosing cholangitis: a pictorial review.Abdom Radiol (NY). 2023 Jan;48(1):63-78. doi: 10.1007/s00261-022-03529-x. Epub 2022 May 14. Abdom Radiol (NY). 2023. PMID: 35567617 Free PMC article. Review.
Cited by
-
Algebraic topology-based machine learning using MRI predicts outcomes in primary sclerosing cholangitis.Eur Radiol Exp. 2022 Nov 18;6(1):58. doi: 10.1186/s41747-022-00312-x. Eur Radiol Exp. 2022. PMID: 36396865 Free PMC article.
-
Clinical utility of 3D magnetic resonance elastography in patients with biliary obstruction.Eur Radiol. 2022 Mar;32(3):2050-2059. doi: 10.1007/s00330-021-08295-w. Epub 2021 Nov 17. Eur Radiol. 2022. PMID: 34791513
-
Primary Sclerosing Cholangitis Risk Estimate Tool (PREsTo) Predicts Outcomes of the Disease: A Derivation and Validation Study Using Machine Learning.Hepatology. 2020 Jan;71(1):214-224. doi: 10.1002/hep.30085. Epub 2018 Dec 28. Hepatology. 2020. PMID: 29742811 Free PMC article.
-
Reporting standards for primary sclerosing cholangitis using MRI and MR cholangiopancreatography: guidelines from MR Working Group of the International Primary Sclerosing Cholangitis Study Group.Eur Radiol. 2022 Feb;32(2):923-937. doi: 10.1007/s00330-021-08147-7. Epub 2021 Aug 6. Eur Radiol. 2022. PMID: 34363134
-
Mildly Low Serum Sodium Levels in Chronic Liver Disease: At Risk for Sarcopenia and Portal Hypertension.Cureus. 2023 Aug 30;15(8):e44419. doi: 10.7759/cureus.44419. eCollection 2023 Aug. Cureus. 2023. PMID: 37664343 Free PMC article.
References
-
- Castera L, Vergniol J, Foucher J, et al. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology. 2005;128:343–350. - PubMed
-
- Corpechot C, El Naggar A, Poujol-Robert A, et al. Assessment of biliary fibrosis by transient elastography in patients with PBC and PSC. Hepatology. 2006;43:1118–1124. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
