

Facial asymmetry: a current review
- PMID: 26691977
- PMCID: PMC4686752
- DOI: 10.1590/2177-6709.20.6.110-125.sar
Facial asymmetry: a current review
Abstract
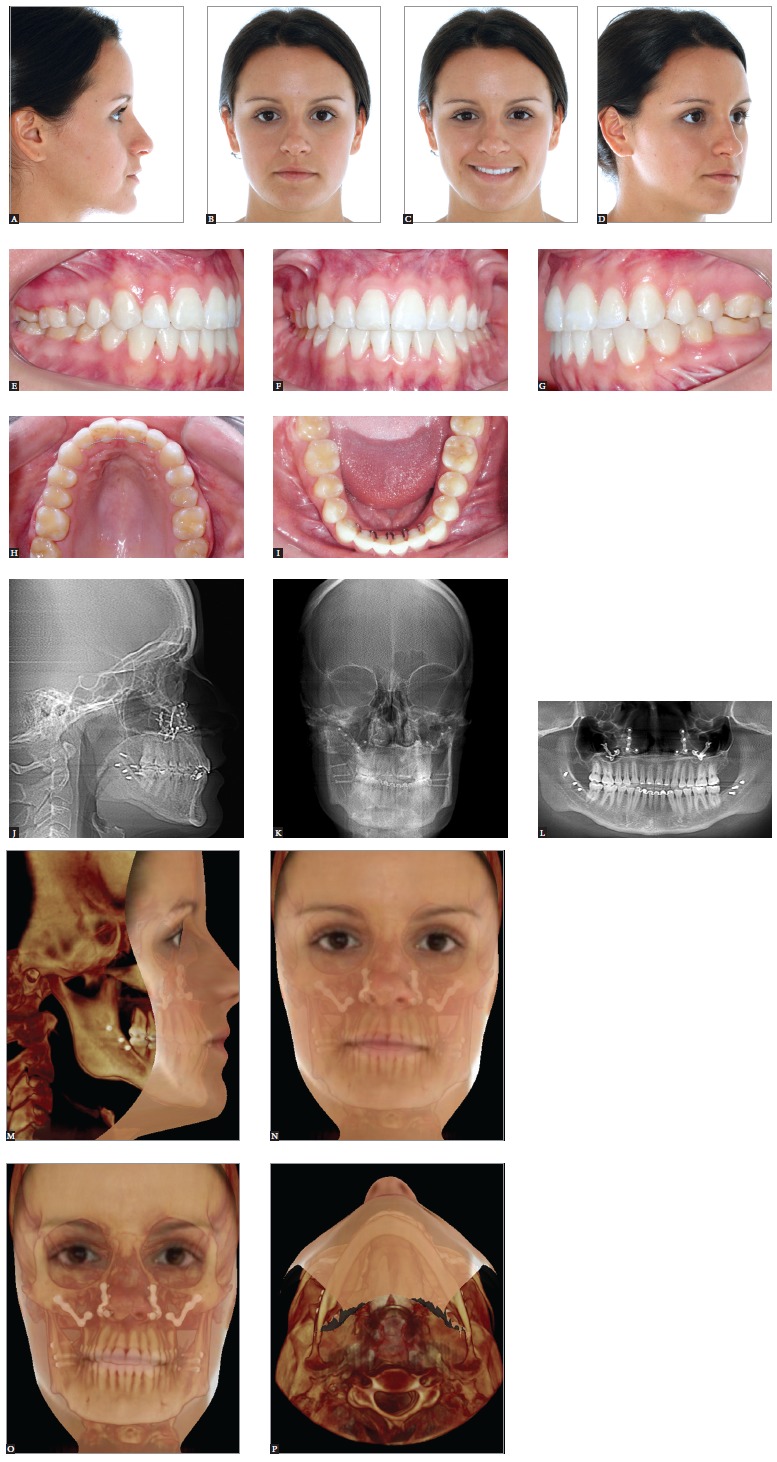
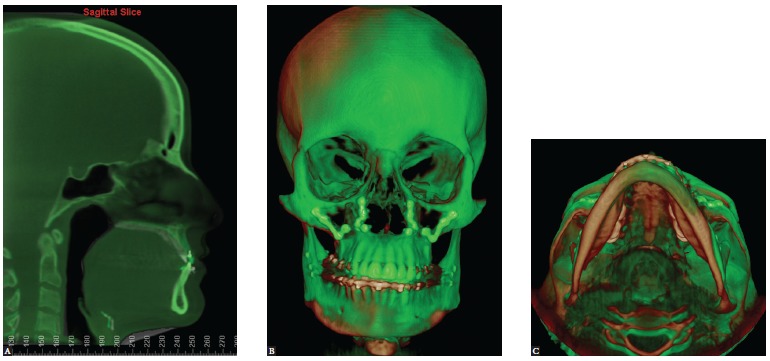
The term "asymmetry" is used to make reference to dissimilarity between homologous elements, altering the balance between structures. Facial asymmetry is common in the overall population and is often presented subclinically. Nevertheless, on occasion, significant facial asymmetry results not only in functional, but also esthetic issues. Under these conditions, its etiology should be carefully investigated in order to achieve an adequate treatment plan. Facial asymmetry assessment comprises patient's first interview, extra- as well as intraoral clinical examination, and supplementary imaging examination. Subsequent asymmetry treatment depends on patient's age, the etiology of the condition and on the degree of disharmony, and might include from asymmetrical orthodontic mechanics to orthognathic surgery. Thus, the present study aims at addressing important aspects to be considered by the orthodontist reaching an accurate diagnosis and treatment plan of facial asymmetry, in addition to reporting treatment of some patients carriers of such challenging disharmony.
O termo assimetria é utilizado quando existe uma desigualdade entre as partes homólogas, afetando, assim, o equilíbrio entre as estruturas. A assimetria facial é comum na população, e muitas vezes se apresenta de forma subclínica. Entretanto, em alguns casos existe uma assimetria facial significativa que resulta tanto em problemas funcionais quanto estéticos. Nessas circunstâncias, a etiologia deve ser cuidadosamente investigada, para que seja possível elaborar um plano de tratamento adequado. A avaliação da assimetria facial é constituída por uma anamnese do paciente, exame clínico extra e intrabucal, além de exames complementares de imagem. O tratamento subsequente dessa assimetria depende da idade do paciente, etiologia e da magnitude da desarmonia, podendo envolver desde mecânicas ortodônticas assimétricas até a realização de cirurgia ortognática. Assim, o presente artigo busca abordar aspectos importantes para que o ortodontista possa realizar um adequado diagnóstico e plano de tratamento da assimetria facial, além de relatar o tratamento de alguns pacientes portadores dessa desafiadora desarmonia.
Figures





References
-
- Lindauer SJ. Asymmetries: diagnosis and treatment (editorial) Semin Orthod. 1998;4(3):133–133. - PubMed
-
- Cheong YW, Lo LJ. Facial asymmetry: etiology, evaluation, and management. Chang Gung Med J. 2011 Jul-Aug;34(4):341–351. - PubMed
-
- IPDTOC Working Group Prevalence at birth of cleft lip with or without cleft palate: data from the International Perinatal Database of Typical Oral Clefts (IPDTOC) Cleft Palate Craniofac J. 2011;48(1):66–81. - PubMed
-
- Peck S, Peck L, Kataja M. Skeletal asymmetry in esthetically pleasing faces. Angle Orthod. 1991;61(1):43–48. - PubMed
-
- Rhodes G, Sumich A, Byatt G. Are Average facial configurations attractive only because of their symmetry. Psychol Sci. 1999;10(1):52–58.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
