

Funding policies and postabortion long-acting reversible contraception: results from a cluster randomized trial
- PMID: 26692178
- PMCID: PMC6005688
- DOI: 10.1016/j.ajog.2015.12.009
Funding policies and postabortion long-acting reversible contraception: results from a cluster randomized trial
Abstract
Background: Almost one-half of women having an abortion in the United States have had a previous procedure, which highlights a failure to provide adequate preventive care. Provision of intrauterine devices and implants, which have high upfront costs, can be uniquely challenging in the abortion care setting.
Objective: We conducted a study of a clinic-wide training intervention on long-acting reversible contraception and examined the effect of the intervention, insurance coverage, and funding policies on the use of long-acting contraceptives after an abortion.
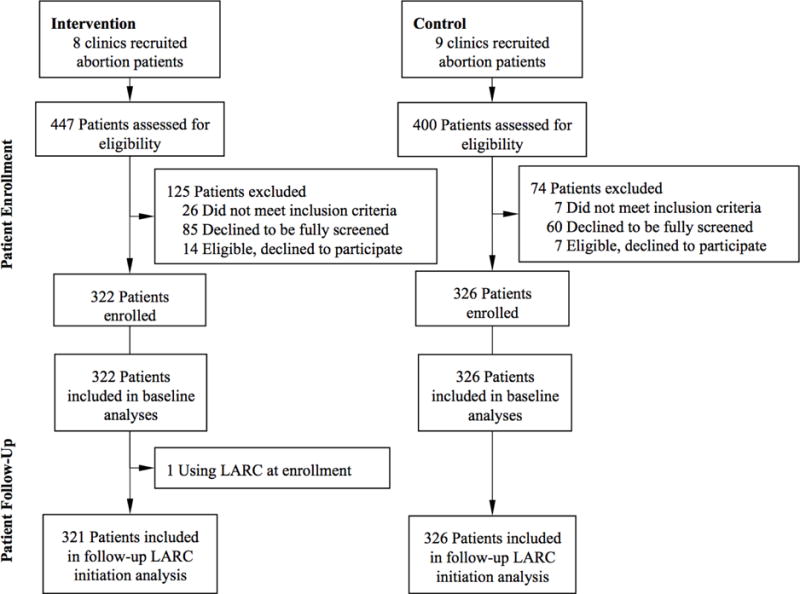
Study design: This subanalysis of a cluster, randomized trial examines data from the 648 patients who had undergone an abortion who were recruited from 17 reproductive health centers across the United States. The trial followed participants 18-25 years old who did not desire pregnancy for a year. We measured the effect of the intervention, health insurance, and funding policies on contraceptive outcomes, which included intrauterine device and implant counseling and selection at the abortion visit, with the use of logistic regression with generalized estimating equations for clustering. We used survival analysis to model the actual initiation of these methods over 1 year.
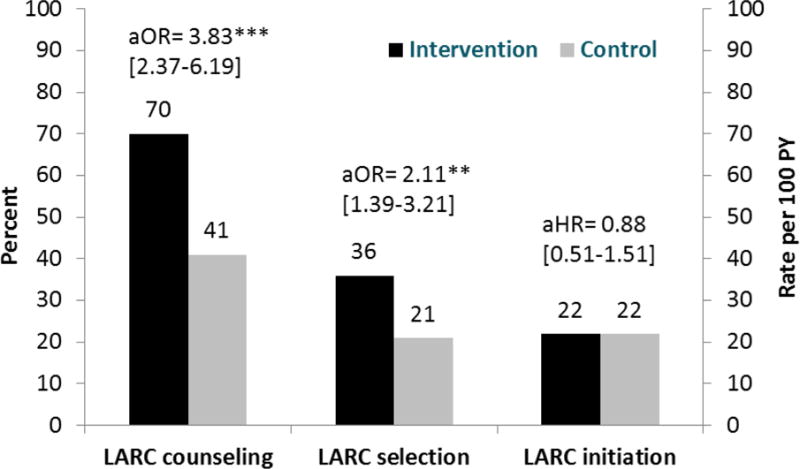
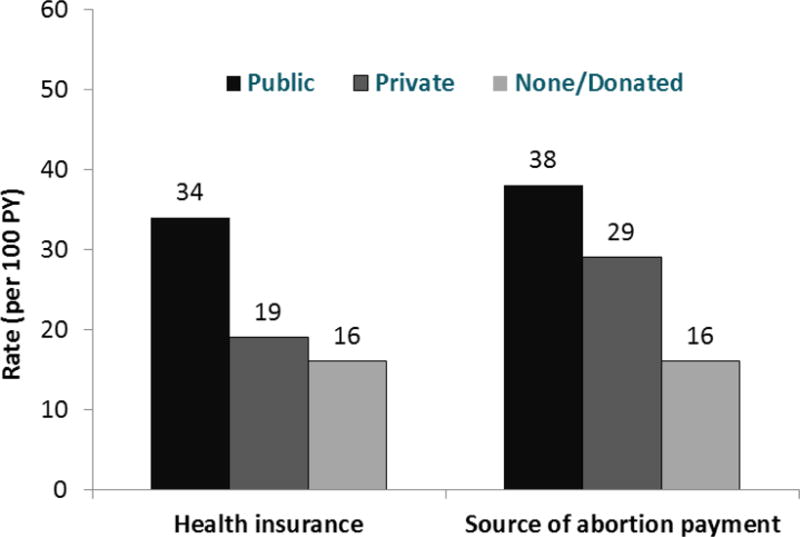
Results: Women who obtained abortion care at intervention sites were more likely to report intrauterine device and implant counseling (70% vs 41%; adjusted odds ratio, 3.83; 95% confidence interval, 2.37-6.19) and the selection of these methods (36% vs 21%; adjusted odds ratio, 2.11; 95% confidence interval, 1.39-3.21). However, the actual initiation of methods was similar between study arms (22/100 woman-years each; adjusted hazard ratio, 0.88; 95% confidence interval, 0.51-1.51). Health insurance and funding policies were important for the initiation of intrauterine devices and implants. Compared with uninsured women, those women with public health insurance had a far higher initiation rate (adjusted hazard ratio, 2.18; 95% confidence interval, 1.31-3.62). Women at sites that provide state Medicaid enrollees abortion coverage also had a higher initiation rate (adjusted hazard ratio, 1.73; 95% confidence interval, 1.04-2.88), as did those at sites with state mandates for private health insurance to cover contraception (adjusted hazard ratio, 1.80; 95% confidence interval, 1.06-3.07). Few of the women with private insurance used it to pay for the abortion (28%), but those who did initiated long-acting contraceptive methods at almost twice the rate as women who paid for it themselves or with donated funds (adjusted hazard ratio, 1.94; 95% confidence interval, 1.10-3.43).
Conclusions: The clinic-wide training increased long-acting reversible contraceptive counseling and selection but did not change initiation for abortion patients. Long-acting method use after abortion was associated strongly with funding. Restrictions on the coverage of abortion and contraceptives in abortion settings prevent the initiation of desired long-acting methods.
Keywords: abortion; insurance; long-acting reversible contraceptive; policy; postabortion contraception.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Contraception after medication abortion in the United States: results from a cluster randomized trial.Am J Obstet Gynecol. 2018 Jan;218(1):107.e1-107.e8. doi: 10.1016/j.ajog.2017.09.020. Epub 2017 Oct 3. Am J Obstet Gynecol. 2018. PMID: 28986072 Free PMC article. Clinical Trial.
-
Postpartum contraception: initiation and effectiveness in a large universal healthcare system.Am J Obstet Gynecol. 2017 Jul;217(1):55.e1-55.e9. doi: 10.1016/j.ajog.2017.02.036. Epub 2017 Feb 28. Am J Obstet Gynecol. 2017. PMID: 28257962
-
Contraceptive discontinuation and pregnancy postabortion in Nepal: a longitudinal cohort study.Contraception. 2015 Apr;91(4):301-7. doi: 10.1016/j.contraception.2014.12.011. Epub 2014 Dec 30. Contraception. 2015. PMID: 25553872
-
Prevention of unintended pregnancy: a focus on long-acting reversible contraception.Prim Care. 2014 Jun;41(2):239-60. doi: 10.1016/j.pop.2014.02.004. Epub 2014 Mar 27. Prim Care. 2014. PMID: 24830607 Review.
-
Contraception After Surgical and Medical Abortion: A Review.Obstet Gynecol Surv. 2017 Aug;72(8):487-493. doi: 10.1097/OGX.0000000000000463. Obstet Gynecol Surv. 2017. PMID: 28817165 Review.
Cited by
-
Long-acting reversible contraception initiation after medication abortion: a retrospective cohort study.Contracept Reprod Med. 2025 May 28;10(1):34. doi: 10.1186/s40834-025-00371-6. Contracept Reprod Med. 2025. PMID: 40437647 Free PMC article.
-
Can youth get the contraception they want? Results of a pilot study in the province of Quebec.Paediatr Child Health. 2020 Apr;25(3):160-165. doi: 10.1093/pch/pxz059. Epub 2019 May 2. Paediatr Child Health. 2020. PMID: 32296277 Free PMC article.
-
Women's Postabortion Contraceptive Preferences and Access to Family Planning Services in Mississippi.Womens Health Issues. 2020 May-Jun;30(3):176-183. doi: 10.1016/j.whi.2020.01.004. Epub 2020 Feb 21. Womens Health Issues. 2020. PMID: 32094055 Free PMC article.
-
Contraceptive Practices, Preferences, and Barriers Among Abortion Clients in North Carolina.South Med J. 2018 Jun;111(6):317-323. doi: 10.14423/SMJ.0000000000000820. South Med J. 2018. PMID: 29863217 Free PMC article.
-
Contraception after medication abortion in the United States: results from a cluster randomized trial.Am J Obstet Gynecol. 2018 Jan;218(1):107.e1-107.e8. doi: 10.1016/j.ajog.2017.09.020. Epub 2017 Oct 3. Am J Obstet Gynecol. 2018. PMID: 28986072 Free PMC article. Clinical Trial.
References
-
- Jones RK, Singh S, Finer LB, Frohwirth LF. Occasional Report No 29. New York, NY: Guttmacher Institute; Nov, 2006. Repeat abortion in the United States. Available at: www.guttmacher.org/pubs/2006/11/21/or29.pdf. Accessed August 8, 2014.
-
- Trussell J. Contraceptive Efficacy. In: Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar MS, editors. Contraceptive Technology. 20th. New York NY: Ardent Media; 2011. pp. 799–863.
-
- Centers for Disease Control and Prevention, Department of Health and Human Services. U.S. Medical Eligibility Criteria for contraceptive use, 2010. MMWR. 2010;59
-
- Grimes D, Schulz K, Stanwood N. Immediate postabortal insertion of intrauterine devices. Cochrane Database Syst Rev. 2004;4:CD001777–CD77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
