

Antibody-Mediated Autoimmune Encephalopathies and Immunotherapies
- PMID: 26692392
- PMCID: PMC4720680
- DOI: 10.1007/s13311-015-0410-6
Antibody-Mediated Autoimmune Encephalopathies and Immunotherapies
Abstract
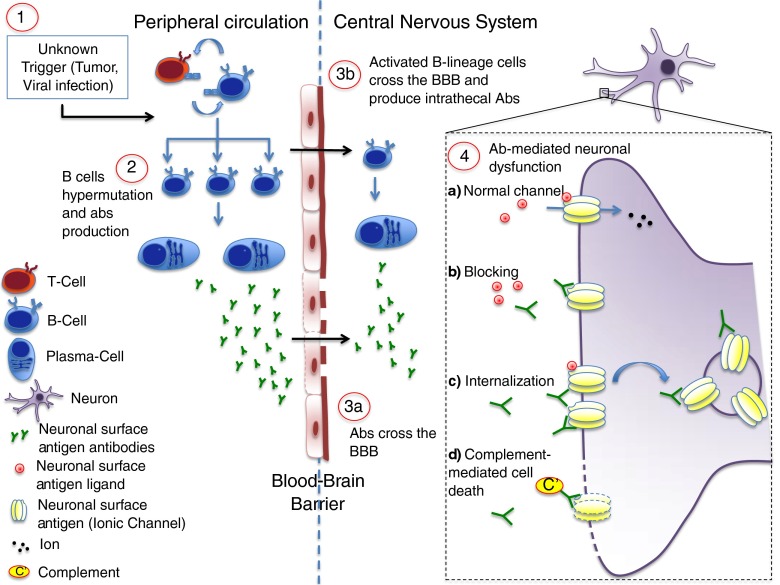
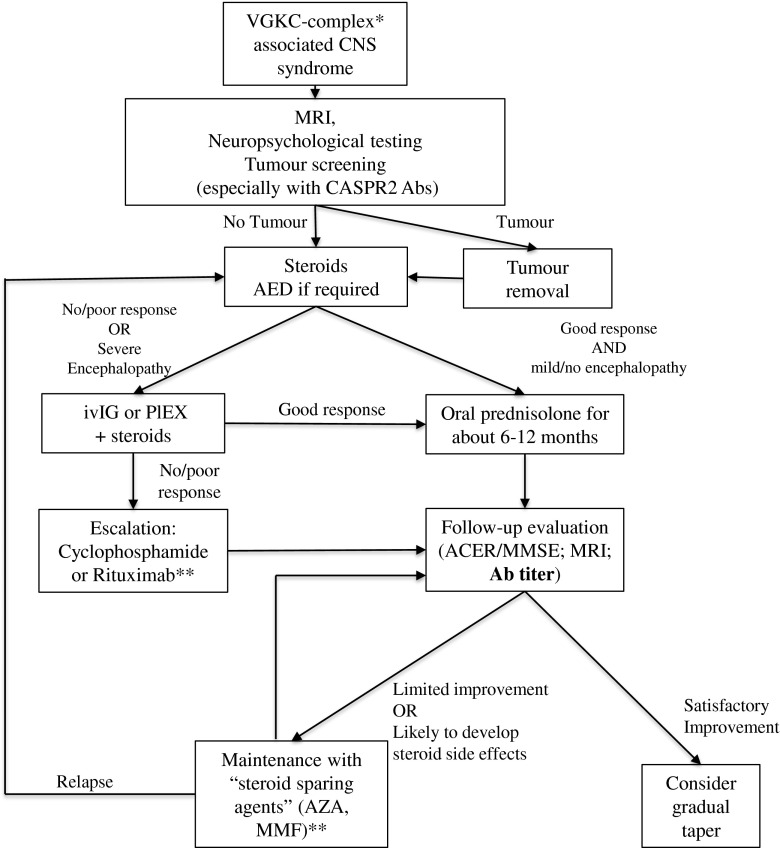
Over the last 15 years it has become clear that rare but highly recognizable diseases of the central nervous system (CNS), including newly identified forms of limbic encephalitis and other encephalopathies, are likely to be mediated by antibodies (Abs) to CNS proteins. The Abs are directed against membrane receptors and ion channel-associated proteins that are expressed on the surface of neurons in the CNS, such as N-methyl D-aspartate receptors and leucine-rich, glioma inactivated 1 protein and contactin-associated protein like 2, that are associated with voltage-gated potassium channels. The diseases are not invariably cancer-related and are therefore different from the classical paraneoplastic neurological diseases that are associated with, but not caused by, Abs to intracellular proteins. Most importantly, the new antibody-associated diseases almost invariably respond to immunotherapies with considerable and sometimes complete recovery, and there is convincing evidence of their pathogenicity in the relatively limited studies performed so far. Treatments include first-line steroids, intravenous immunoglobulins, and plasma exchange, and second-line rituximab and cyclophosphamide, followed in many cases by steroid-sparing agents in the long-term. This review focuses mainly on N-methyl D-aspartate receptor- and voltage-gated potassium channel complex-related Abs in adults, the clinical phenotypes, and treatment responses. Pediatric cases are referred to but not reviewed in detail. As there have been very few prospective studies, the conclusions regarding immunotherapies are based on retrospective studies.
Keywords: Autoantibodies; Autoimmune encephalopathy; Immunosuppressive treatment; N-methyl D-aspartate receptor; Voltage-gated potassium channel-complex.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
