

Collaborative care for comorbid depression and coronary heart disease: a systematic review and meta-analysis of randomised controlled trials
- PMID: 26692557
- PMCID: PMC4691772
- DOI: 10.1136/bmjopen-2015-009128
Collaborative care for comorbid depression and coronary heart disease: a systematic review and meta-analysis of randomised controlled trials
Abstract
Objectives: To systematically review the efficacy of collaborative care (CC) for depression in adults with coronary heart disease (CHD) and depression.
Design: Systematic review and meta-analysis.
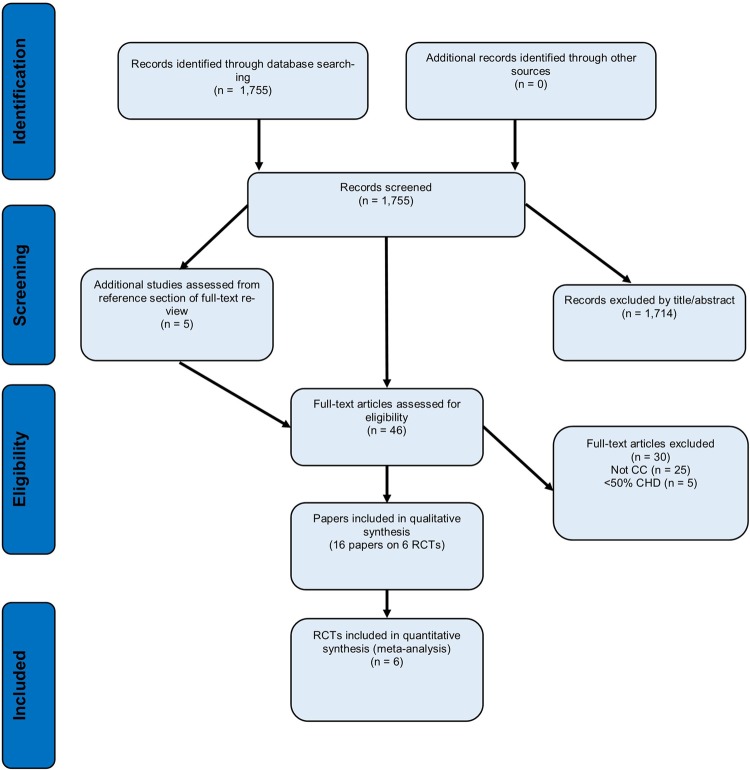
Data sources: Electronic databases (Cochrane Central Register of Controlled Trials MEDLINE, EMBASE, PsycINFO and CINAHL) were searched until April 2014.
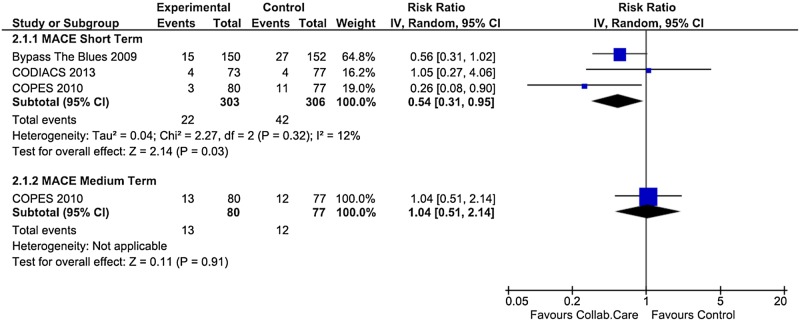
Inclusion criteria: Population, depression comorbid with CHD; intervention, randomised controlled trial (RCT) of CC; comparison, either usual care, wait-list control group or no further treatment; and outcome, (primary) major adverse cardiac events (MACE), (secondary) standardised measure of depression, anxiety, quality of life (QOL) and cost-effectiveness.
Data extraction and analysis: RevMan V.5.3 was used to synthesise the data as risk ratios (RRs), ORs and standardised mean differences (SMD) with 95% CIs in random effect models.
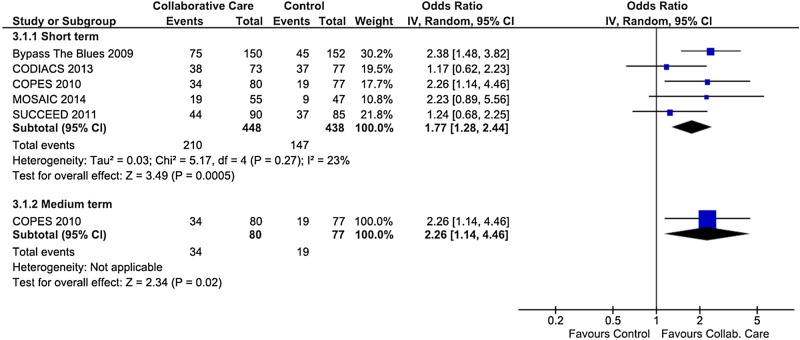
Results: Six RCTs met the inclusion criteria and comprised 655 participants randomised to CC and 629 participants randomised to the control group (total 1284). Collaborative depression care led to a significant reduction in MACE in the short term (three trials, RR 0.54; 95% CI 0.31 to 0.95, p=0.03) that was not sustained in the longer term. Small reductions in depressive symptoms were evident in the short term (6 trials, pooled SMD -0.31; 95% CI -0.43 to -0.19, p<0.00001) and depression remission was more likely to be achieved with CC (5 trials, OR 1.77; 95% CI 1.28 to 2.44, p=0.0005). Likewise, a significant effect was observed for anxiety symptoms (SMD -0.36) and mental QOL (SMD 0.24). The timing of the intervention was a source of between-group heterogeneity for depression symptoms (between groups p=0.04, I(2)=76.5%).
Conclusions: Collaborative depression care did not lead to a sustained reduction in the primary MACE end point. Small effects were observed for depression, depression remission, anxiety and mental QOL.
Trials registration number: PROSPERO CRD42014013653.
Keywords: CARDIOLOGY; MENTAL HEALTH.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures

References
-
- Lichtman JH, Froelicher ES, Blumenthal JA et al. . Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation 2014;129:1350–69. 10.1161/CIR.0000000000000019 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous