

Abdominal anatomy in the context of port placement and trocars
- PMID: 26692776
- PMCID: PMC4664217
- DOI: 10.5152/jtgga.2015.0148
Abdominal anatomy in the context of port placement and trocars
Abstract
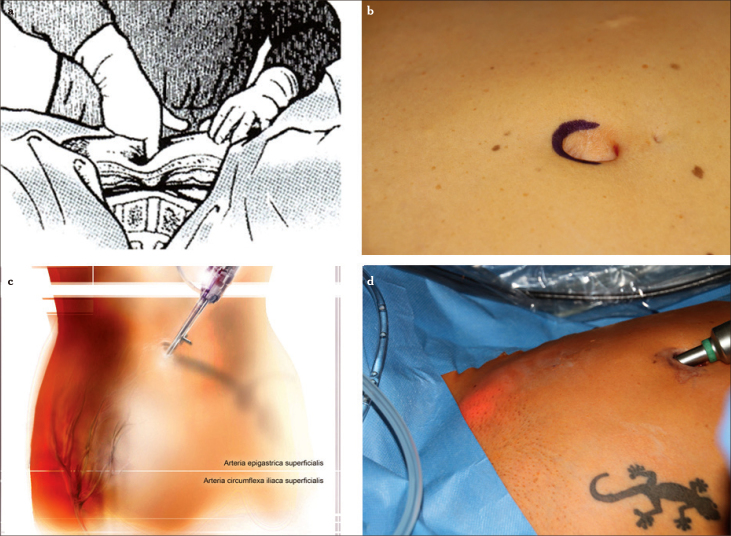
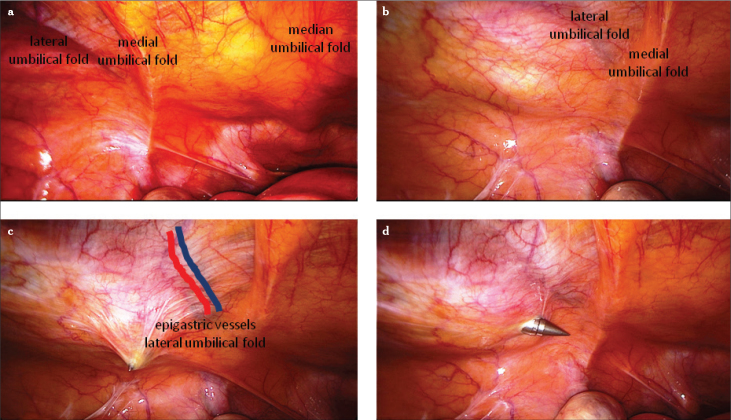
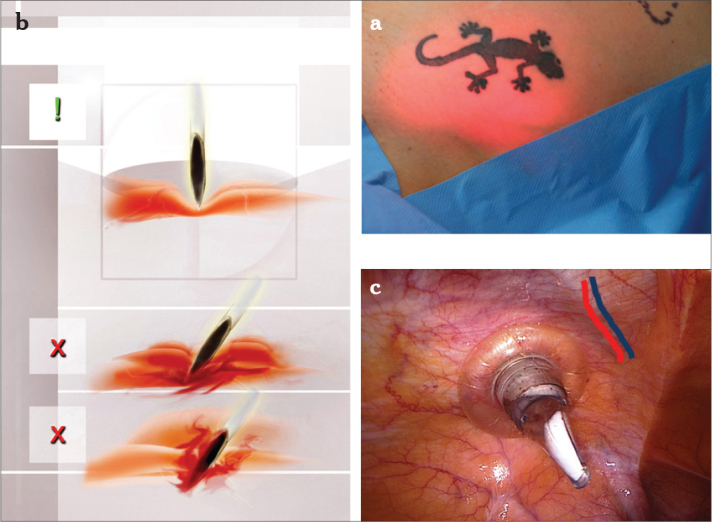
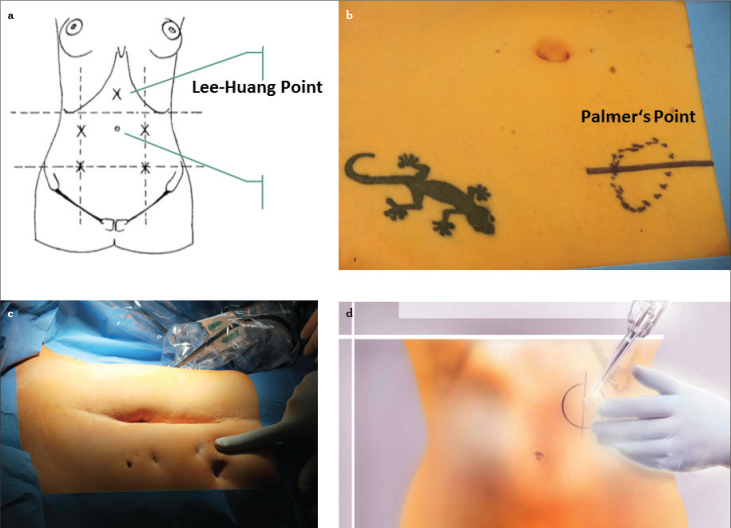
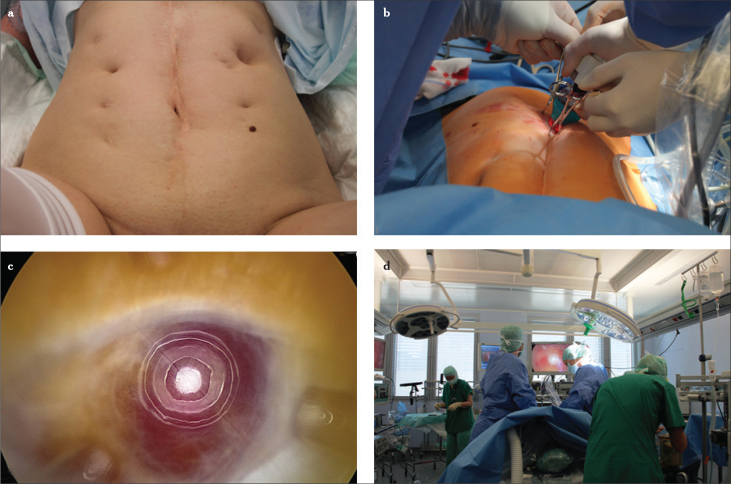
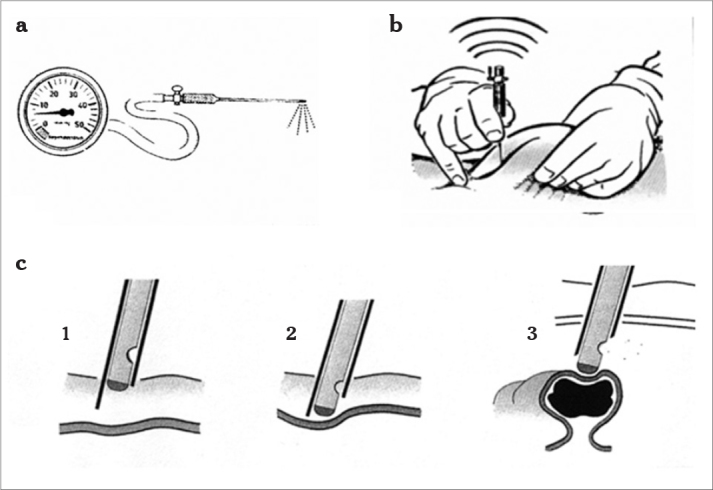
Although the anatomy of the human being has not changed, technical developments in operating materials and methods demand a simultaneous development in operative management. Developments in electronic and optical technologies permit many gynecological operations to be performed laparoscopically. One fundamental distinction between any other operating method and laparoscopy is the hurdle that the initial entry, whether with a needle, cannula, or trocar, is mostly performed blind. However, there is a risk that blind entry may result in vascular or organ damage. One of the difficulties associated with entry complications is that any damage may not be immediately recognized, leading to major abdominal reparative surgery, and at worst, a temporary colostomy. Therefore, the technical and operative quality of laparoscopic surgery begins with port placement and trocars. Visual access systems are available but are not yet widely used. The aim of this review was to introduce the different port placement and trocar systems as well as their correct and professional usage in correlation with the abdominal functional anatomy.
Keywords: Gynecological endoscopy; complication prevention; entry technique; functional gynecological anatomy; pneumoperitoneum; port placement.
Figures



Similar articles
-
Laparoscopic entry: a review of techniques, technologies, and complications.J Obstet Gynaecol Can. 2007 May;29(5):433-447. doi: 10.1016/S1701-2163(16)35496-2. J Obstet Gynaecol Can. 2007. PMID: 17493376 Review. English, French.
-
Complications of Laparoscopy in Connection with Entry Techniques.J Gynecol Surg. 2017 Jun 1;33(3):81-91. doi: 10.1089/gyn.2016.0111. J Gynecol Surg. 2017. PMID: 28663686 Free PMC article. Review.
-
[Risks associated with laparoscopic entry].J Gynecol Obstet Biol Reprod (Paris). 2010 Dec;39(8 Suppl 2):S123-35. doi: 10.1016/S0368-2315(10)70039-9. J Gynecol Obstet Biol Reprod (Paris). 2010. PMID: 21185465 French.
-
Use of the optical access trocar for safe and rapid entry in various laparoscopic procedures.Surg Endosc. 2001 Jun;15(6):570-3. doi: 10.1007/s004640080056. Epub 2001 Apr 3. Surg Endosc. 2001. PMID: 11591942
-
The role of optical access trocars in laparoscopic surgery.Surg Technol Int. 2005;14:61-7. Surg Technol Int. 2005. PMID: 16525956 Review.
Cited by
-
The first robotic-assisted hysterectomy below the bikini line with the Dexter robotic system™.Facts Views Vis Obgyn. 2024 Mar;16(1):87-91. doi: 10.52054/FVVO.16.1.010. Facts Views Vis Obgyn. 2024. PMID: 38551479 Free PMC article.
-
Complications in laparoscopic and robotic-assisted surgery: definitions, classifications, incidence and risk factors - an up-to-date review.Wideochir Inne Tech Maloinwazyjne. 2021 Sep;16(3):501-525. doi: 10.5114/wiitm.2021.108800. Epub 2021 Aug 28. Wideochir Inne Tech Maloinwazyjne. 2021. PMID: 34691301 Free PMC article. Review.
-
Robotic Surgery Techniques to Improve Traditional Laparoscopy.JSLS. 2022 Apr-Jun;26(2):e2022.00002. doi: 10.4293/JSLS.2022.00002. JSLS. 2022. PMID: 35655469 Free PMC article. Review.
-
Preperitoneal insufflation pressure of the abdominal wall in a porcine model.Surg Endosc. 2022 Jan;36(1):300-306. doi: 10.1007/s00464-020-08275-z. Epub 2021 Jan 22. Surg Endosc. 2022. PMID: 33481111
-
The Blooming phenomenon: a rarity, but a dilemma in hysteroscopic resection of myomas.J Turk Ger Gynecol Assoc. 2022 Mar 8;23(1):63-67. doi: 10.4274/jtgga.galenos.2021.2021.0006. Epub 2021 Jun 4. J Turk Ger Gynecol Assoc. 2022. PMID: 34082489 Free PMC article.
References
-
- Alkatout I, Bojahr B, Dittmann L, Warneke V, Mettler L, Jonat W, Schollmeyer T. Precarious preoperative diagnostics and hints for the laparoscopic excision of uterine adenomatoid tumors: two exemplary cases and literature review. Fertil Steril. 2011;95:1119 e5–8. - PubMed
-
- Alkatout I, Honemeyer U, Strauss A, Tinelli A, Malvasi A, Jonat W, et al. Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv. 2013;68:571–81. http://dx.doi.org/10.1097/OGX.0b013e31829cdbeb. - DOI - PubMed
-
- Alkatout I, Stuhlmann-Laeisz C, Mettler L, Jonat W, Schollmeyer T. Organ-preserving management of ovarian pregnancies by laparoscopic approach. Fertil Steril. 2011;95:2467–70. e1–2. - PubMed
-
- Levine R. Instrumentation and equipment. In: Pasic R, Levine R, editors. A practical Manual of Laparoscopy: A Clinical Cookbook. Abingdon, UK: Informa Healthcare; 2007. pp. 19–38. http://dx.doi.org/10.3109/9781439804315. - DOI
-
- Alkatout I, Mettler L, Beteta C, Hedderich J, Jonat W, Schollmeyer T, Salmassi A. Combined surgical and hormone therapy for endometriosis is the most effective treatment: prospective, randomized, controlled trial. J Minim Invasive Gynecol. 2013;20:473–81. http://dx.doi.org/10.1016/j.jmig.2013.01.019. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources