

Offloading treatment is linked to activation of proinflammatory cytokines and start of bone repair and remodeling in Charcot arthropathy patients
- PMID: 26692902
- PMCID: PMC4676128
- DOI: 10.1186/s13047-015-0129-y
Offloading treatment is linked to activation of proinflammatory cytokines and start of bone repair and remodeling in Charcot arthropathy patients
Abstract
Background: Proinflammatory cytokines are an integral part of the osteolytic activity of Charcot arthropathy but are also central to normal bone healing. As there are no previous longitudinal studies investigating their role during the recovery phase of Charcot, we set out to monitor systemic levels of proinflammatory cytokines from Charcot presentation until a clinically and radiographically documented chronic state has been reached.
Methods: Twenty-eight consecutive Charcot patients were monitored during 2 years by repeated foot radiographs, MRI and plasma levels of interleukin [IL]-6, IL-8, IL-1β, Tumor Necrosis Factor [TNF]-α, and IL-1 receptor antibody (IL-1RA). Charcot patients were treated with total contact cast (TCC) on the first day of inclusion. Neuropathic diabetic controls (n = 20) and Healthy subjects (n = 20) served as reference.
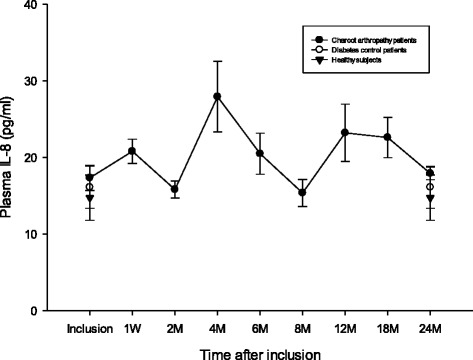
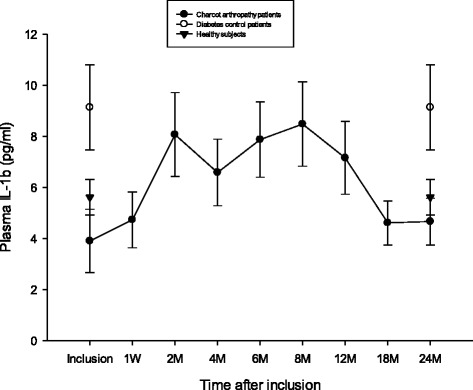
Results: Plasma IL-6, IL-8, IL-1β and TNF-α in the acute and chronic phase of Charcot were below or at the level of diabetic controls and healthy, whereas IL-1RA/IL-1β ratio was continuously higher in Charcot patients. IL-6, TNF-α and IL-1RA began to increase one week after offloading to reach a peak after 4 months before gradually receding.
Conclusions: A sustained increase of IL-6 and TNF-α starting shortly after offloading and paralleled by accelerated bone healing on radiographs, suggest that offloading, by activating the inflammatory stage, has a key role to play in the onset of coupled bone remodeling. High IL-1RA/IL-1β ratio in Charcot patients at presentation supports a counter-balancing anti-inflammatory role for IL-1RA in the acute phase whereas a high ratio after two years, possibly due to renewed weight-bearing on a deformed foot, signal need for continued anti-inflammatory activity and contradicts a "cold" biological state in the chronic phase.
Keywords: Bone healing; Charcot arthropathy; Charcot foot; Diabetes; Fracture; IL-1 receptor antibody; IL-1beta; IL-6; IL-8; Neuropathy; Offloading; Proinflammatory cytokines; TNF-alpha.
Figures





References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
