

Heterogeneity of glucagonomas due to differential processing of proglucagon-derived peptides
- PMID: 26693280
- PMCID: PMC4685488
- DOI: 10.1530/EDM-15-0105
Heterogeneity of glucagonomas due to differential processing of proglucagon-derived peptides
Abstract
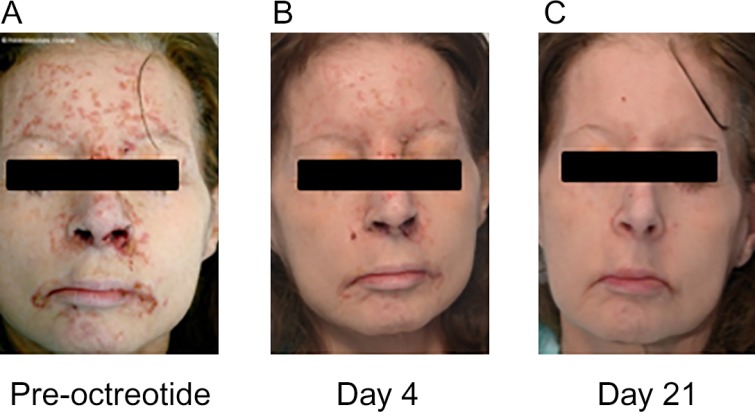
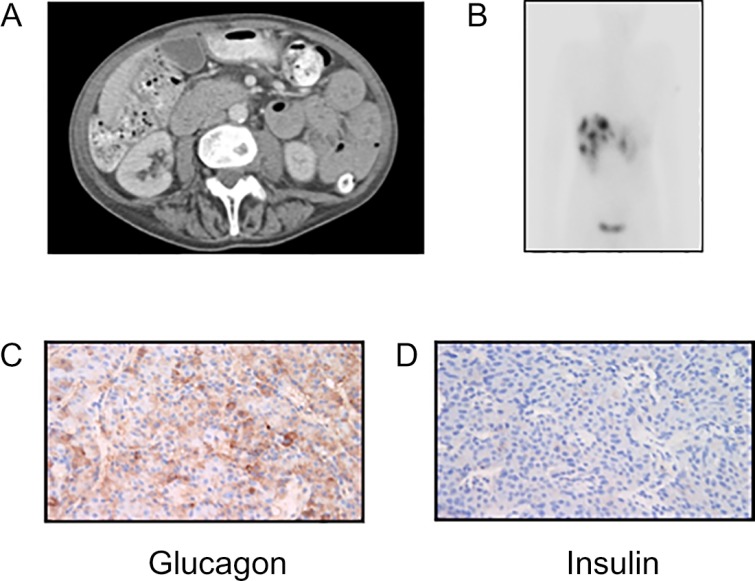
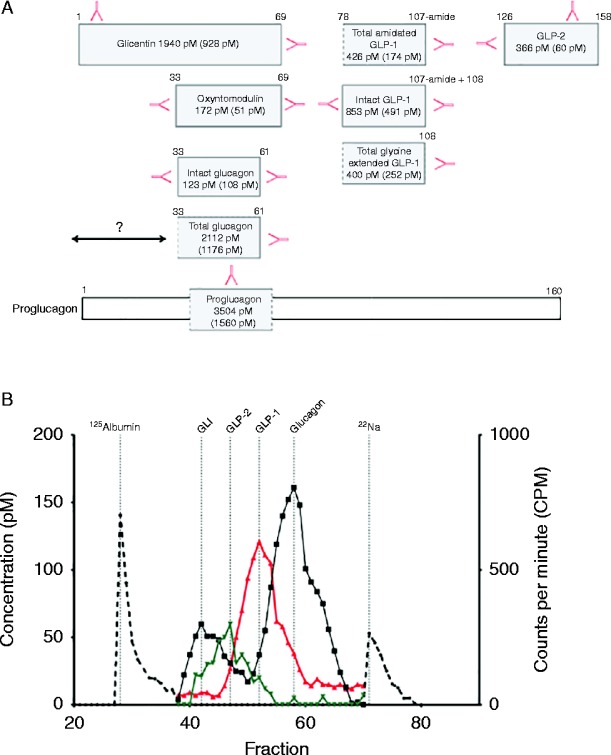
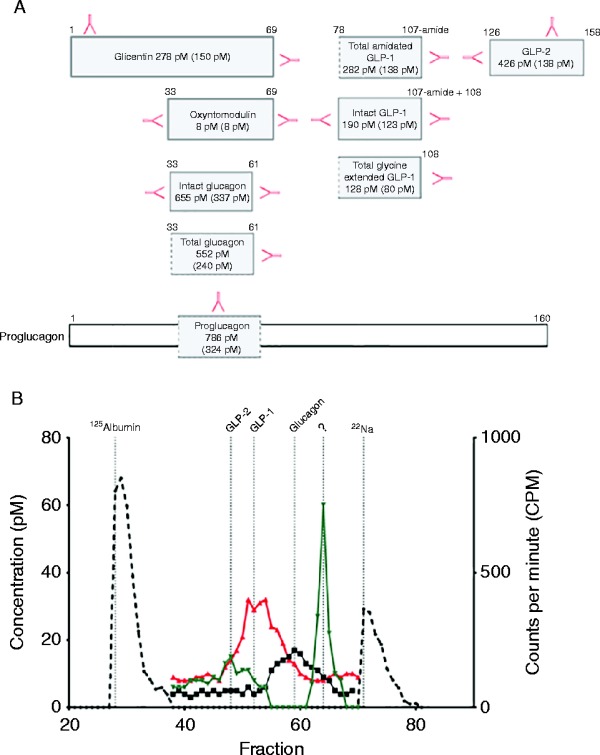
Pancreatic neuroendocrine tumours (pNETs) secreting proglucagon are associated with phenotypic heterogeneity. Here, we describe two patients with pNETs and varied clinical phenotypes due to differential processing and secretion of proglucagon-derived peptides (PGDPs). Case 1, a 57-year-old woman presented with necrolytic migratory erythema, anorexia, constipation and hyperinsulinaemic hypoglycaemia. She was found to have a grade 1 pNET, small bowel mucosal thickening and hyperglucagonaemia. Somatostatin analogue (SSA) therapy improved appetite, abolished hypoglycaemia and improved the rash. Case 2, a 48-year-old male presented with diabetes mellitus, diarrhoea, weight loss, nausea, vomiting and perineal rash due to a grade 1 metastatic pNET and hyperglucagonaemia. In both cases, plasma levels of all measured PGDPs were elevated and attenuated following SSA therapy. In case 1, there was increased production of intact glucagon-like peptide 1 (GLP-1) and GLP-2, similar to that of the enteroendocrine L cell. In case 2, pancreatic glucagon was elevated due to a pancreatic α-cell-like proglucagon processing profile. In summary, we describe two patients with pNETs and heterogeneous clinical phenotypes due to differential processing and secretion of PGDPs. This is the first description of a patient with symptomatic hyperinsulinaemic hypoglycaemia and marked gastrointestinal dysfunction due to, in part, a proglucagon-expressing pNET.
Learning points: PGDPs exhibit a diverse range of biological activities including critical roles in glucose and amino acid metabolism, energy homeostasis and gastrointestinal physiology.The clinical manifestations of proglucagon-expressing tumours may exhibit marked phenotypic variation due to the biochemical heterogeneity of their secreted peptide repertoire.Specific and precise biochemical assessment of individuals with proglucagon-expressing tumours may provide opportunities for improved diagnosis and clinical management.
Figures
References
-
- Ellingsgaard H, Hauselmann I, Schuler B, Habib AM, Baggio LL, Meier DT, Eppler E, Bouzakri K, Wueest S, Muller YD et al. 2011. Interleukin-6 enhances insulin secretion by increasing glucagon-like peptide-1 secretion from L cells and α cells. Nature Medicine 17 1481–1489. 10.1038/nm.2513 - DOI - PMC - PubMed
-
- Roberts RE, Zhao M, Whitelaw BC, Ramage J, Diaz-Cano S, Roux CWI, Quaglia A, Huang GC & Aylwin SJB. 2012. GLP-1 and glucagon secretion from a pancreatic neuroendocrine tumor causing diabetes and hyperinsulinemic hypoglycemia. Journal of Clinical Endocrinology and Metabolism 97 3039–3045. 10.1210/jc.2011-2005 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
