

Intra-cardiac echocardiography in alcohol septal ablation: a prospective comparative study against trans-thoracic echocardiography
- PMID: 26693311
- PMCID: PMC4676484
- DOI: 10.1530/ERP-15-0002
Intra-cardiac echocardiography in alcohol septal ablation: a prospective comparative study against trans-thoracic echocardiography
Abstract
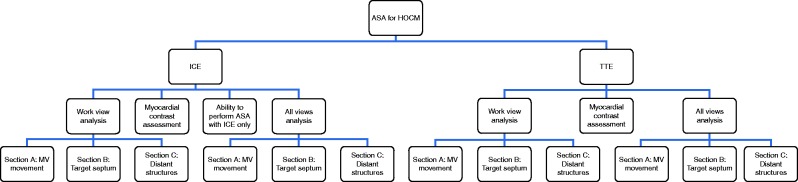
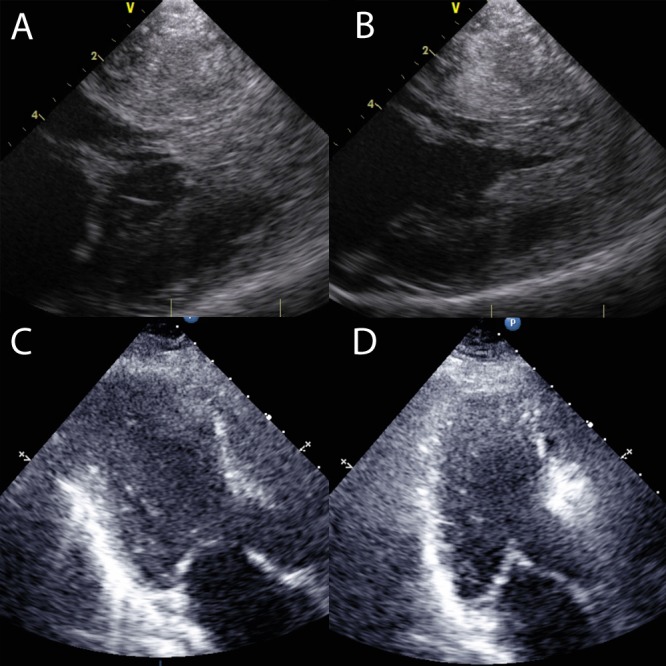
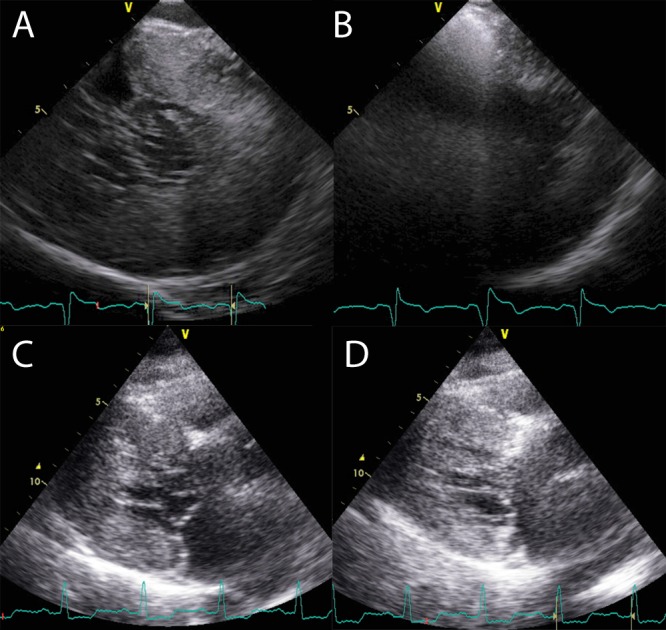
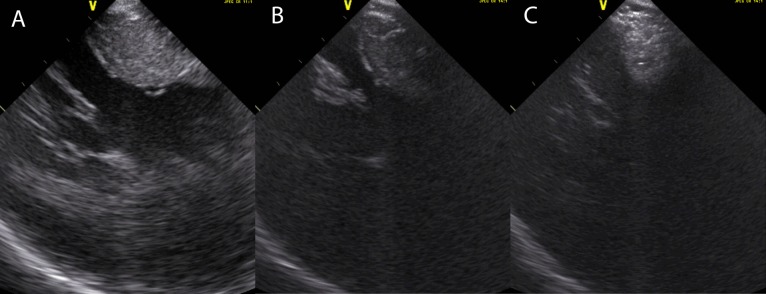
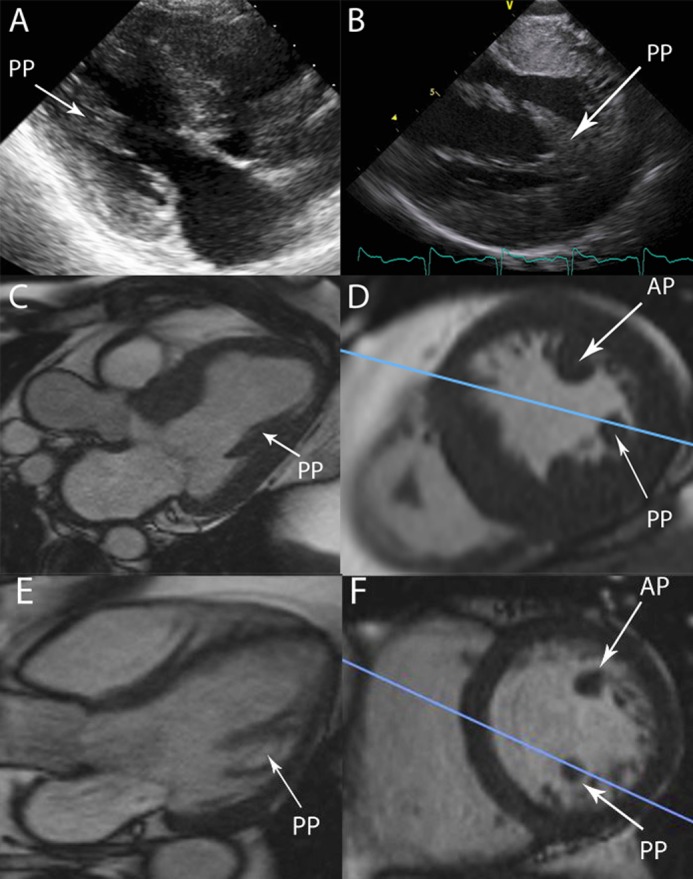
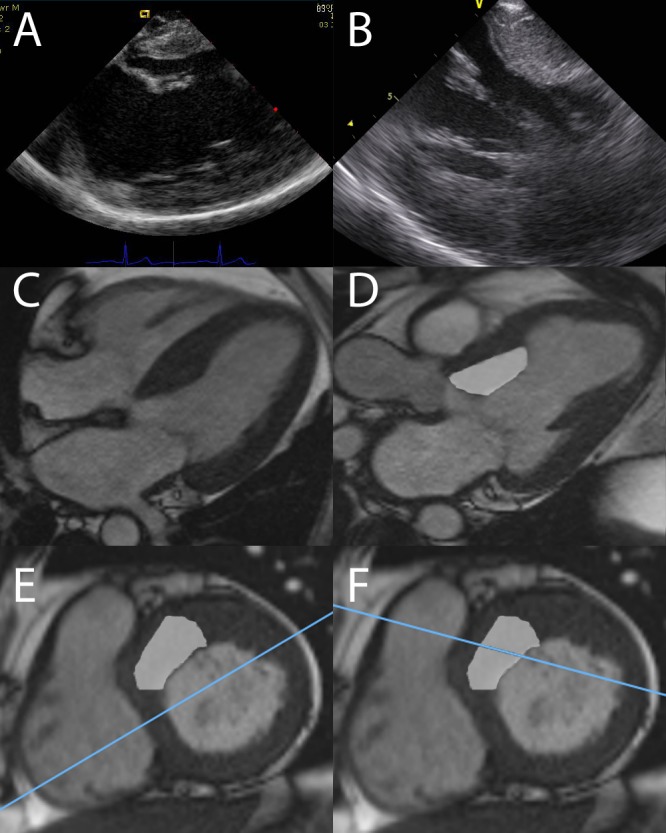
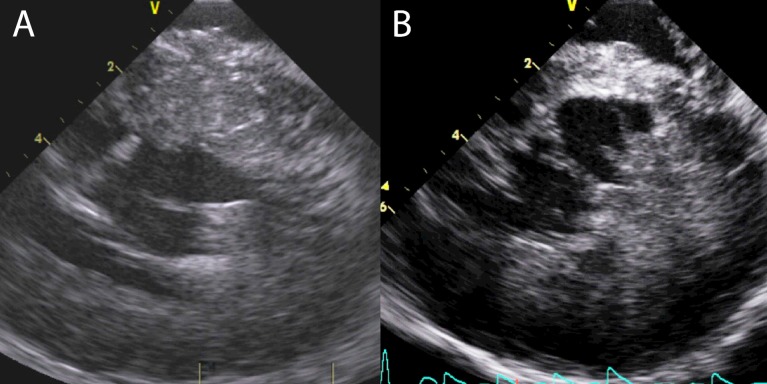
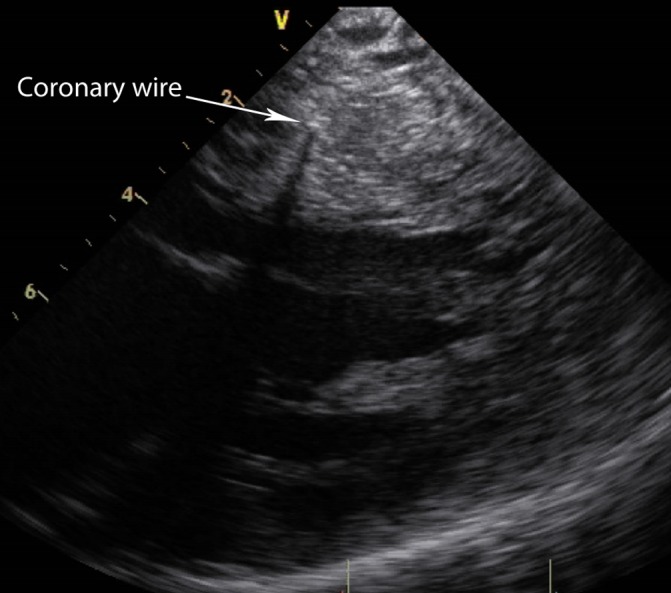
Alcohol septal ablation (ASA) in hypertrophic obstructive cardiomyopathy reduces left ventricular outflow tract gradients. A third of patients do not respond; inaccurate localisation of the iatrogenic infarct can be responsible. Transthoracic echocardiography (TTE) using myocardial contrast can be difficult in the laboratory environment. Intra-cardiac echocardiography (ICE) provides high-quality images. We aimed to assess ICE against TTE in ASA. The ability of ICE and TTE to assess three key domains (mitral valve (MV) anatomy and systolic anterior motion, visualisation of target septum, adjacent structures) was evaluated in 20 consecutive patients undergoing ASA. Two independent experts scored paired TTE and ICE images off line for each domain in both groups. The ability to see myocardial contrast following septal arterial injection was also assessed by the cardiologist performing ASA. In patients undergoing ASA, ICE was superior in viewing MV anatomy (P=0.02). TTE was superior in assessing adjacent structures (P=0.002). There was no difference in assessing target septum. Myocardial contrast: ICE did not clearly identify the area of contrast in 17/19 patients due to dense acoustic shadowing (8/19) and inadequate opacification of the myocardium (6/19). ICE only clearly localised contrast in 2/19 cases. ICE does not visualise myocardial contrast well and therefore cannot be used to guide ASA. TTE was substantially better at viewing myocardial contrast. There was no significant difference between ICE and TTE in the overall ability to comment on cardiac anatomy relevant to ASA.
Keywords: alcohol septal ablation; hypertrophic obstructive cardiomyopathy; non-surgical septal reduction therapy.
Figures
Similar articles
-
Radiofrequency ablation of the interventricular septum to treat outflow tract gradients in hypertrophic obstructive cardiomyopathy: a novel use of CARTOSound® technology to guide ablation.Europace. 2016 Jan;18(1):113-20. doi: 10.1093/europace/euv302. Epub 2015 Nov 4. Europace. 2016. PMID: 26541709
-
Reduction of left ventricular mass, left atrial size, and N-terminal pro-B-type natriuretic peptide level following alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy.Kardiol Pol. 2019;77(2):181-189. doi: 10.5603/KP.a2018.0242. Epub 2018 Dec 19. Kardiol Pol. 2019. PMID: 30566209
-
An assessment of regression of left ventricular hypertrophy following alcohol ablation of the interventricular septum in patients with hypertrophic cardiomyopathy with left ventricular outflow tract obstruction.Kardiol Pol. 2012;70(8):782-8. Kardiol Pol. 2012. PMID: 22933209
-
Intervention in HCM: patient selection, procedural approach and emerging techniques in alcohol septal ablation.Echo Res Pract. 2015 Mar 1;2(1):R25-35. doi: 10.1530/ERP-14-0058. Epub 2014 Oct 30. Echo Res Pract. 2015. PMID: 26693329 Free PMC article. Review.
-
Intracardiac echocardiography guidance for alcohol septal ablation in hypertrophic obstructive cardiomyopathy.J Invasive Cardiol. 2007 May;19(5):E134-6. J Invasive Cardiol. 2007. PMID: 17470972 Review.
Cited by
-
Role of endocardial septal ablation in the treatment of hypertrophic obstructive cardiomyopathy.Anatol J Cardiol. 2016 Sep;16(9):707-12. doi: 10.14744/AnatolJCardiol.2016.7100. Anatol J Cardiol. 2016. PMID: 27609434 Free PMC article. Review.
-
Intracardiac echocardiography Chinese expert consensus.Front Cardiovasc Med. 2022 Oct 6;9:1012731. doi: 10.3389/fcvm.2022.1012731. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36277762 Free PMC article. Review.
-
Effective alcohol septal ablation for left ventricular outflow tract obstruction in a patient with isolated dextrocardia.BMJ Case Rep. 2019 Nov 28;12(11):e231922. doi: 10.1136/bcr-2019-231922. BMJ Case Rep. 2019. PMID: 31780619 Free PMC article.
