

Vital Signs Directed Therapy: Improving Care in an Intensive Care Unit in a Low-Income Country
- PMID: 26693728
- PMCID: PMC4687915
- DOI: 10.1371/journal.pone.0144801
Vital Signs Directed Therapy: Improving Care in an Intensive Care Unit in a Low-Income Country
Abstract
Background: Global Critical Care is attracting increasing attention. At several million deaths per year, the worldwide burden of critical illness is greater than generally appreciated. Low income countries (LICs) have a disproportionally greater share of critical illness, and yet critical care facilities are scarce in such settings. Routines utilizing abnormal vital signs to identify critical illness and trigger medical interventions have become common in high-income countries but have not been investigated in LICs. The aim of the study was to assess whether the introduction of a vital signs directed therapy protocol improved acute care and reduced mortality in an Intensive Care Unit (ICU) in Tanzania.
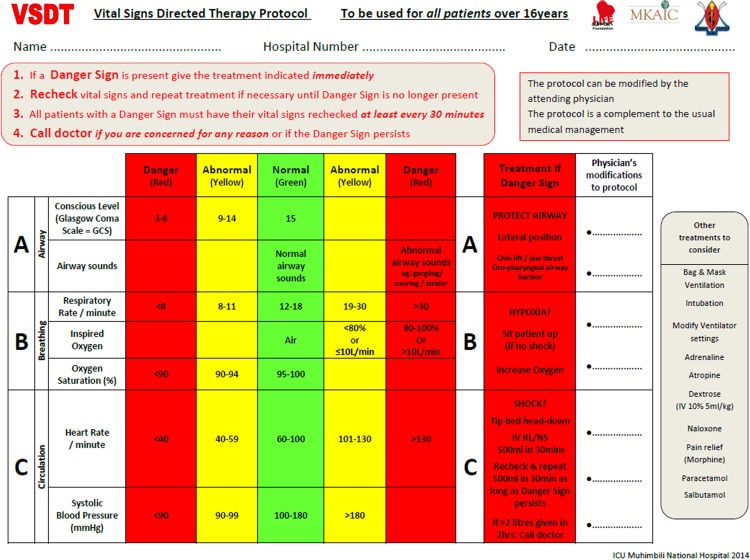
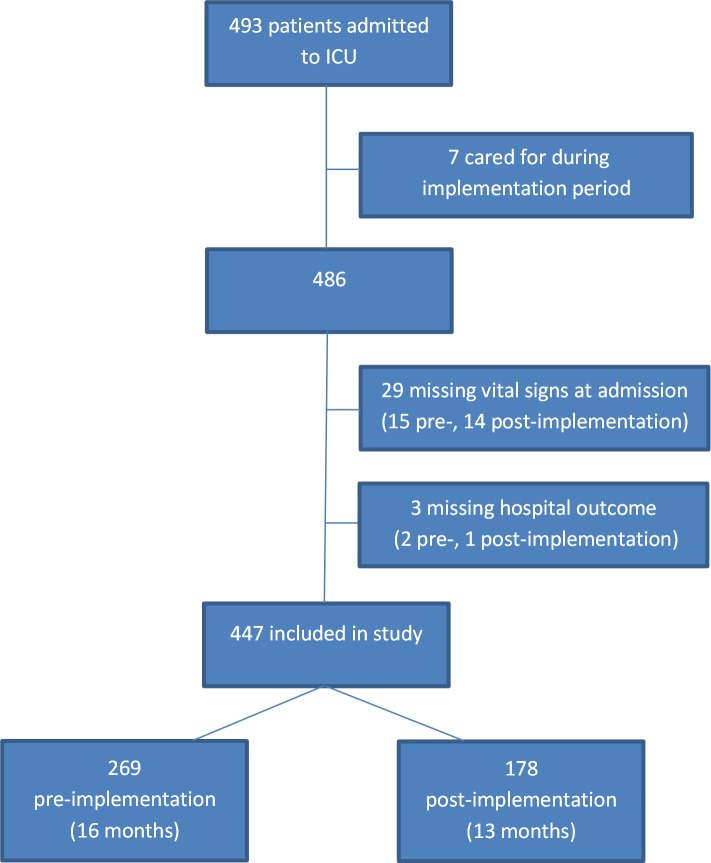
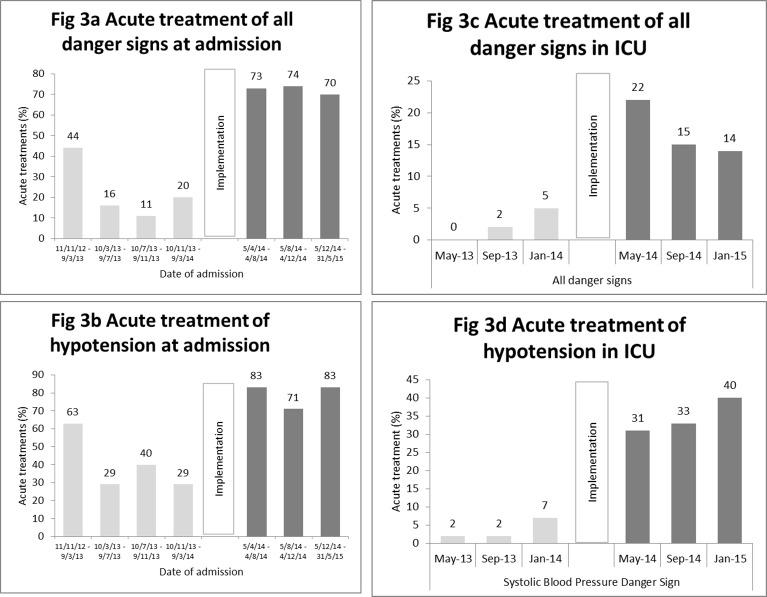
Methods and findings: Prospective, before-and-after interventional study in the ICU of a university hospital in Tanzania. A context-appropriate protocol that defined danger levels of severely abnormal vital signs and stipulated acute treatment responses was implemented in a four week period using sensitisation, training, job aids, supervision and feedback. Acute treatment of danger signs at admission and during care in the ICU and in-hospital mortality were compared pre and post-implementation using regression models. Danger signs from 447 patients were included: 269 pre-implementation and 178 post-implementation. Acute treatment of danger signs was higher post-implementation (at admission: 72.9% vs 23.1%, p<0.001; in ICU: 16.6% vs 2.9%, p<0.001). A danger sign was five times more likely to be treated post-implementation (Prevalence Ratio (PR) 4.9 (2.9-8.3)). Intravenous fluids were given in response to 35.0% of hypotensive episodes post-implementation, as compared to 4.1% pre-implementation (PR 6.4 (2.5-16.2)). In patients admitted with hypotension, mortality was lower post-implementation (69.2% vs 92.3% p = 0.02) giving a numbers-needed-to-treat of 4.3. Overall in-hospital mortality rates were unchanged (49.4% vs 49.8%, p = 0.94).
Conclusion: The introduction of a vital signs directed therapy protocol improved the acute treatment of abnormal vital signs in an ICU in a low-income country. Mortality rates were reduced for patients with hypotension at admission but not for all patients.
Conflict of interest statement
Figures
References
-
- Meara JG, Leather AJ, Hagander L, Alkire BC, Alonso N, Ameh EA, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015. - PubMed
-
- Mock C, Kobusingye O, Joshipura M, Nguyen S, Arreola-Risa C. Strengthening trauma and critical care globally. Current opinion in critical care. 2005;11(6):568–75. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
