

Arteriovenous Fistula Development in the First 6 Weeks after Creation
- PMID: 26694050
- PMCID: PMC4851120
- DOI: 10.1148/radiol.2015150385
Arteriovenous Fistula Development in the First 6 Weeks after Creation
Abstract
Purpose: To assess the anatomic development of native arteriovenous fistula (AVF) during the first 6 weeks after creation by using ultrasonographic (US) measurements in a multicenter hemodialysis fistula maturation study.
Materials and methods: Each institutional review board approved the prospective study protocol, and written informed consent was obtained. Six hundred and two participants (180 women and 422 men, 459 with upper-arm AVF and 143 with forearm AVF) from seven clinical centers underwent preoperative artery and vein US mapping. AVF draining vein diameter and blood flow rate were assessed postoperatively after 1 day, 2 weeks, and 6 weeks. Relationships among US measurements were summarized after using multiple imputation for missing measurements.
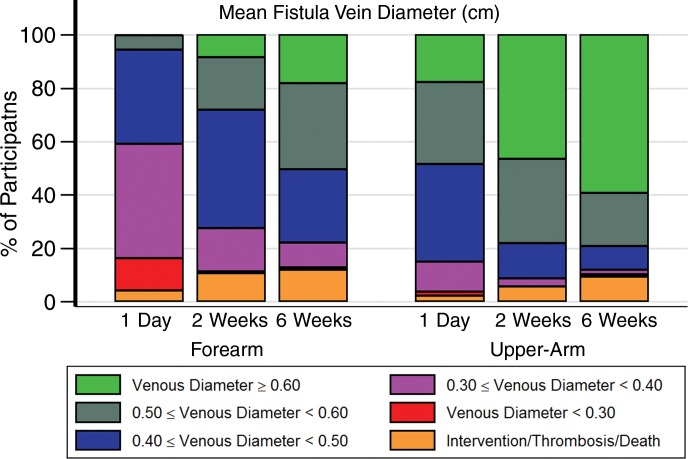
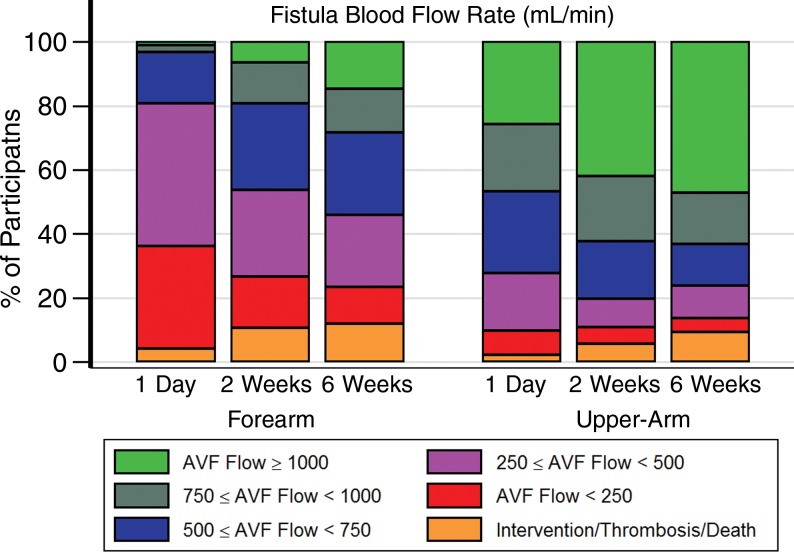
Results: In 55% of forearm AVFs (68 of 124) and 83% of upper-arm AVFs (341 of 411) in surviving patients without thrombosis or AVF intervention prior to 6 weeks, at least 50% of their 6-week blood flow rate measurement was achieved at 1 day. Among surviving patients without thrombosis or AVF intervention prior to week 2, 70% with upper-arm AVFs (302 of 433) and 77% with forearm AVFs (99 of 128) maintained at least 85% of their week 2 flow rate at week 6. Mean AVF diameters of at least 0.40 cm were seen in 85% (389 of 459), 91% (419 of 459), and 87% (401 of 459) of upper-arm AVFs and in 40% (58 of 143), 73% (104 of 143), and 77% (110 of 143) of forearm AVFs at 1 day, 2 weeks, and 6 weeks, respectively. One-day and 2-week AVF flow rates and diameters were used to predict 6-week levels, with 2-week prediction of 6-week measures more accurate than those of 1 day (flow rates, R(2) = 0.47 and 0.61, respectively; diameters, R(2) = 0.49 and 0.82, respectively).
Conclusion: AVF blood flow rate at 1 day is usually more than 50% of the 6-week blood flow rate. Two-week measurements are more predictive of 6-week diameter and blood flow than those of 1 day. US measurements at 2 weeks may be of value in the early identification of fistulas that are unlikely to develop optimally.
(©) RSNA, 2015 Online supplemental material is available for this article.
Figures


References
-
- Wong V, Ward R, Taylor J, Selvakumar S, How TV, Bakran A. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg 1996;12(2):207–213. - PubMed
-
- Mahmutyazicioğlu K, Kesenci M, Fitöz S, Büyükberber S, Sencan O, Erden I. Hemodynamic changes in the early phase of artificially created arteriovenous fistula: color Doppler ultrasonographic findings. J Ultrasound Med 1997;16(12):813–817. - PubMed
-
- Malovrh M. Non-invasive evaluation of vessels by duplex sonography prior to construction of arteriovenous fistulas for haemodialysis. Nephrol Dial Transplant 1998;13(1):125–129. - PubMed
-
- Lomonte C, Casucci F, Antonelli M, et al. . Is there a place for duplex screening of the brachial artery in the maturation of arteriovenous fistulas? Semin Dial 2005;18(3):243–246. - PubMed
-
- Allon M, Robbin ML. Increasing arteriovenous fistulas in hemodialysis patients: problems and solutions. Kidney Int 2002;62(4):1109–1124. - PubMed
Publication types
MeSH terms
Grants and funding
- U01DK082240/DK/NIDDK NIH HHS/United States
- U01DK082179/DK/NIDDK NIH HHS/United States
- U01 DK082218/DK/NIDDK NIH HHS/United States
- U01DK082222/DK/NIDDK NIH HHS/United States
- U01 DK082232/DK/NIDDK NIH HHS/United States
- U01DK082218/DK/NIDDK NIH HHS/United States
- U01 DK082240/DK/NIDDK NIH HHS/United States
- U01 DK066597/DK/NIDDK NIH HHS/United States
- U01 DK082179/DK/NIDDK NIH HHS/United States
- U01 DK082222/DK/NIDDK NIH HHS/United States
- U01DK066597/DK/NIDDK NIH HHS/United States
- U01 DK082236/DK/NIDDK NIH HHS/United States
- U01DK082189/DK/NIDDK NIH HHS/United States
- U01 DK082189/DK/NIDDK NIH HHS/United States
- U01DK082236/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
