

Risks and Benefits of Nalmefene in the Treatment of Adult Alcohol Dependence: A Systematic Literature Review and Meta-Analysis of Published and Unpublished Double-Blind Randomized Controlled Trials
- PMID: 26694529
- PMCID: PMC4687857
- DOI: 10.1371/journal.pmed.1001924
Risks and Benefits of Nalmefene in the Treatment of Adult Alcohol Dependence: A Systematic Literature Review and Meta-Analysis of Published and Unpublished Double-Blind Randomized Controlled Trials
Abstract
Background: Nalmefene is a recent option in alcohol dependence treatment. Its approval was controversial. We conducted a systematic review and meta-analysis of the aggregated data (registered as PROSPERO 2014:CRD42014014853) to compare the harm/benefit of nalmefene versus placebo or active comparator in this indication.
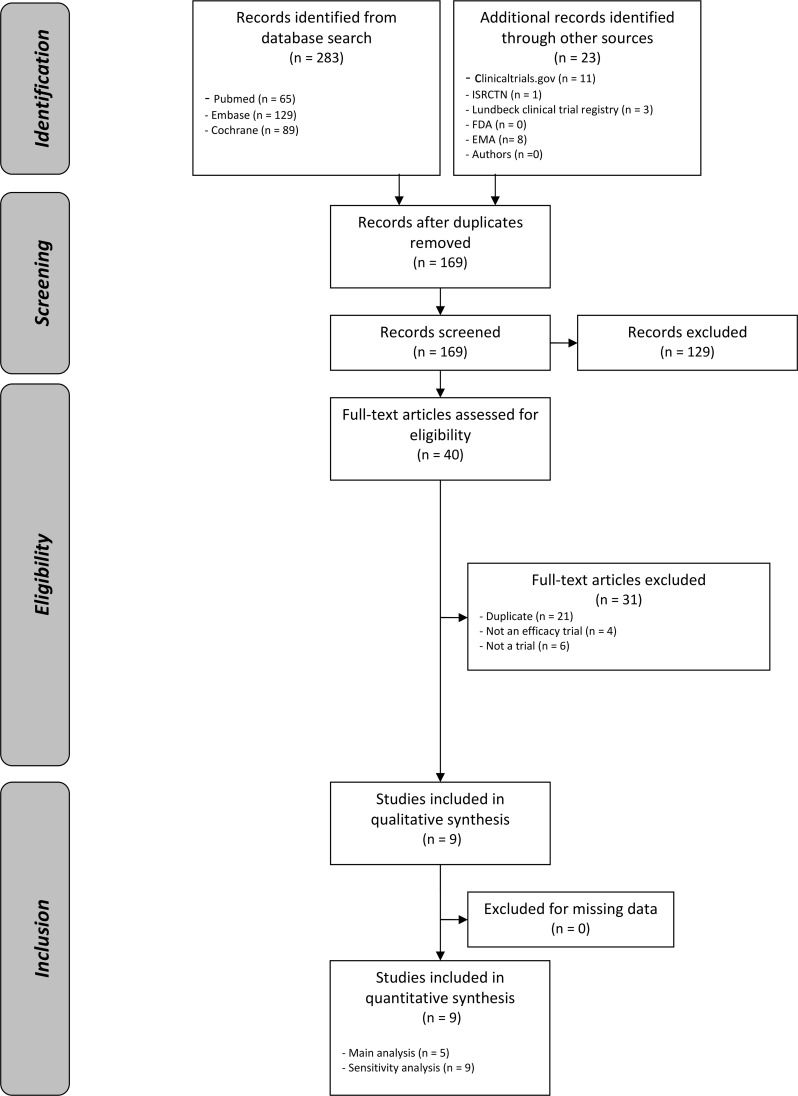
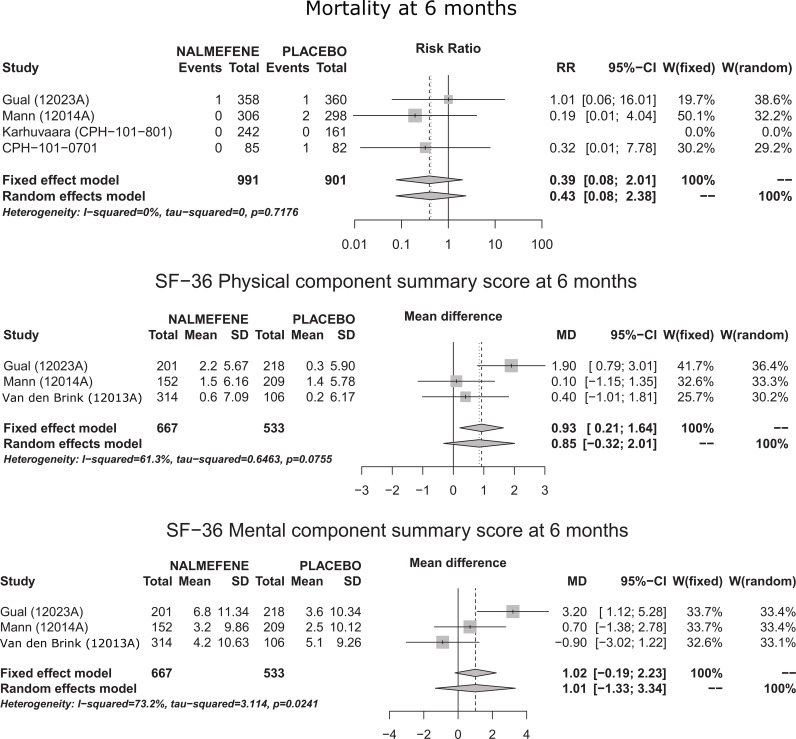
Methods and findings: Three reviewers searched for published and unpublished studies in Medline, the Cochrane Library, Embase, ClinicalTrials.gov, Current Controlled Trials, and bibliographies and by mailing pharmaceutical companies, the European Medicines Agency (EMA), and the US Food and Drug Administration. Double-blind randomized clinical trials evaluating nalmefene to treat adult alcohol dependence, irrespective of the comparator, were included if they reported (1) health outcomes (mortality, accidents/injuries, quality of life, somatic complications), (2) alcohol consumption outcomes, (3) biological outcomes, or (4) treatment safety outcomes, at 6 mo and/or 1 y. Three authors independently screened the titles and abstracts of the trials identified. Relevant trials were evaluated in full text. The reviewers independently assessed the included trials for methodological quality using the Cochrane Collaboration tool for assessing risk of bias. On the basis of the I2 index or the Cochrane's Q test, fixed or random effect models were used to estimate risk ratios (RRs), mean differences (MDs), or standardized mean differences (SMDs) with 95% CIs. In sensitivity analyses, outcomes for participants who were lost to follow-up were included using baseline observation carried forward (BOCF); for binary measures, patients lost to follow-up were considered equal to failures (i.e., non-assessed patients were recorded as not having responded in both groups). Five randomized controlled trials (RCTs) versus placebo, with a total of 2,567 randomized participants, were included in the main analysis. None of these studies was performed in the specific population defined by the EMA approval of nalmefene, i.e., adults with alcohol dependence who consume more than 60 g of alcohol per day (for men) or more than 40 g per day (for women). No RCT compared nalmefene with another medication. Mortality at 6 mo (RR = 0.39, 95% CI [0.08; 2.01]) and 1 y (RR = 0.98, 95% CI [0.04; 23.95]) and quality of life at 6 mo (SF-36 physical component summary score: MD = 0.85, 95% CI [-0.32; 2.01]; SF-36 mental component summary score: MD = 1.01, 95% CI [-1.33; 3.34]) were not different across groups. Other health outcomes were not reported. Differences were encountered for alcohol consumption outcomes such as monthly number of heavy drinking days at 6 mo (MD = -1.65, 95% CI [-2.41; -0.89]) and at 1 y (MD = -1.60, 95% CI [-2.85; -0.35]) and total alcohol consumption at 6 mo (SMD = -0.20, 95% CI [-0.30; -0.10]). An attrition bias could not be excluded, with more withdrawals for nalmefene than for placebo, including more withdrawals for safety reasons at both 6 mo (RR = 3.65, 95% CI [2.02; 6.63]) and 1 y (RR = 7.01, 95% CI [1.72; 28.63]). Sensitivity analyses showed no differences for alcohol consumption outcomes between nalmefene and placebo, but the weight of these results should not be overestimated, as the BOCF approach to managing withdrawals was used.
Conclusions: The value of nalmefene for treatment of alcohol addiction is not established. At best, nalmefene has limited efficacy in reducing alcohol consumption.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Meta-analysis finds no evidence for efficacy of nalmefene in treating alcohol dependence.BMJ. 2015 Dec 29;351:h6988. doi: 10.1136/bmj.h6988. BMJ. 2015. PMID: 26715052 No abstract available.
References
-
- Marlatt GA, Witkiewitz K. Harm reduction approaches to alcohol use: health promotion, prevention, and treatment. Addict Behav. 2002;27:867–886. - PubMed
-
- European Medicines Agency. Assessment report: Selincro—international non-proprietory name: nalmefene. EMA/78844/2013. 13 Dec 2012. Available: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_asses.... Accessed 16 November 2015.
-
- National Institute for Health and Care Excellence. Nalmefene for reducing alcohol consumption in people with alcohol dependence: evaluation report London: National Institute for Health and Care Excellence; 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
