

A decision tree to assess short-term mortality after an emergency department visit for an exacerbation of COPD: a cohort study
- PMID: 26695935
- PMCID: PMC4699373
- DOI: 10.1186/s12931-015-0313-4
A decision tree to assess short-term mortality after an emergency department visit for an exacerbation of COPD: a cohort study
Abstract
Background: Creating an easy-to-use instrument to identify predictors of short-term (30/60-day) mortality after an exacerbation of chronic obstructive pulmonary disease (eCOPD) could help clinicians choose specific measures of medical care to decrease mortality in these patients. The objective of this study was to develop and validate a classification and regression tree (CART) to predict short term mortality among patients evaluated in an emergency department (ED) for an eCOPD.
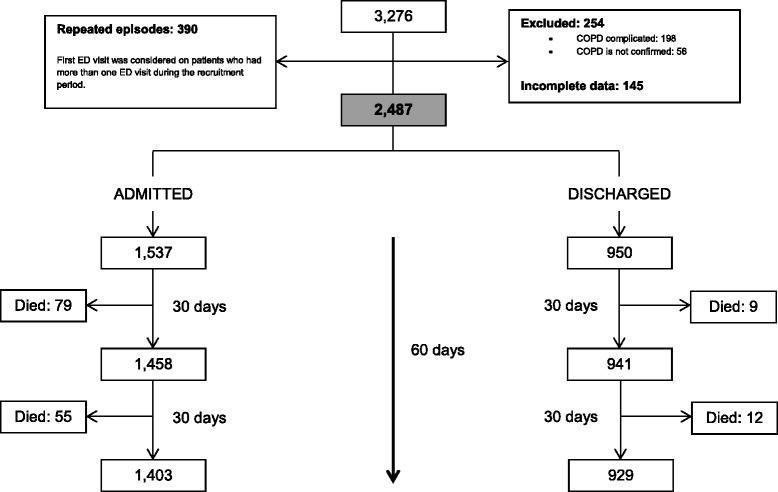
Methods: We conducted a prospective cohort study including participants from 16 hospitals in Spain. COPD patients with an exacerbation attending the emergency department (ED) of any of the hospitals between June 2008 and September 2010 were recruited. Patients were randomly divided into derivation (50%) and validation samples (50%). A CART based on a recursive partitioning algorithm was created in the derivation sample and applied to the validation sample.
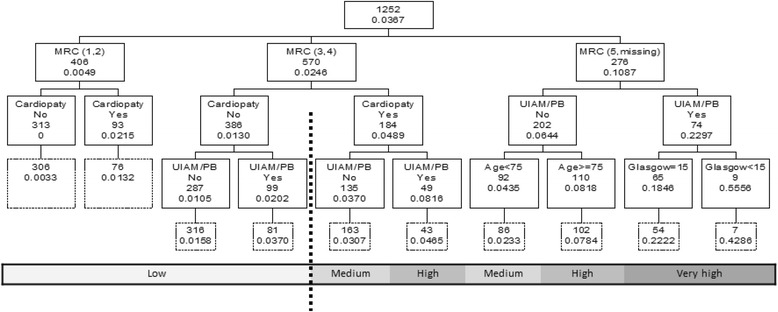
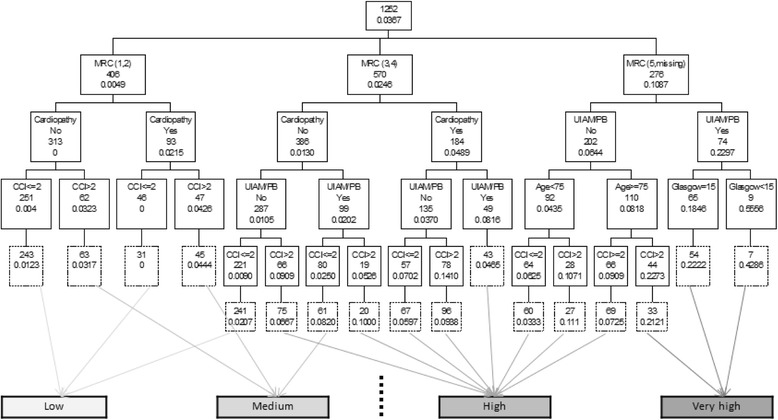
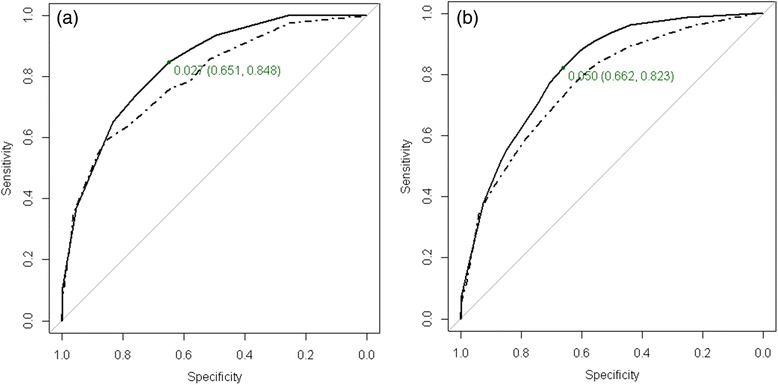
Results: Two thousand four hundred eighty-seven patients, 1252 patients in the derivation sample and 1235 in the validation sample, were enrolled in the study. Based on the results of the univariate analysis, five variables (baseline dyspnea, cardiac disease, the presence of paradoxical breathing or use of accessory inspiratory muscles, age, and Glasgow Coma Scale score) were used to build the CART. Mortality rates 30 days after discharge ranged from 0% to 55% in the five CART classes. The lowest mortality rate was for the branch composed of low baseline dyspnea and lack of cardiac disease. The highest mortality rate was in the branch with the highest baseline dyspnea level, use of accessory inspiratory muscles or paradoxical breathing upon ED arrival, and Glasgow score <15. The area under the receiver-operating curve (AUC) in the derivation sample was 0.835 (95% CI: 0.783, 0.888) and 0.794 (95% CI: 0.723, 0.865) in the validation sample. CART was improved to predict 60-days mortality risk by adding the Charlson Comorbidity Index, reaching an AUC in the derivation sample of 0.817 (95% CI: 0.776, 0.859) and 0.770 (95% CI: 0.716, 0.823) in the validation sample.
Conclusions: We identified several easy-to-determine variables that allow clinicians to classify eCOPD patients by short term mortality risk, which can provide useful information for establishing appropriate clinical care.
Trial registration: NCT02434536.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
