

Recurrent venous thromboembolism and abnormal uterine bleeding with anticoagulant and hormone therapy use
- PMID: 26696010
- PMCID: PMC4832477
- DOI: 10.1182/blood-2015-08-665927
Recurrent venous thromboembolism and abnormal uterine bleeding with anticoagulant and hormone therapy use
Abstract
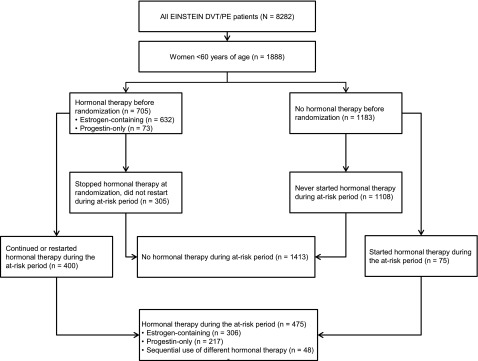
Women receiving vitamin K antagonists (VKAs) require adequate contraception because of the potential for fetal complications. It is unknown whether the use of hormonal therapy, especially those containing estrogens, is associated with recurrent venous thromboembolism (VTE) during anticoagulation. Despite the absence of data, World Health Organization guidelines state that use of estrogen-containing contraceptives confers an "unacceptable health risk" during established anticoagulation for VTE. We compared the incidences of recurrent VTE and abnormal uterine bleeding with and without concomitant hormonal therapy in women aged <60 years who were receiving anticoagulation with rivaroxaban or enoxaparin/VKA for confirmed VTE. Incidence densities in percentage per year were computed for the on and off estrogen-containing or progestin-only therapy periods. Cox regression models were fitted, with hormonal therapy (on vs off) as a time-dependent variable to derive the hazard ratio (HR) for the effects on recurrent VTE and abnormal uterine bleeding. In total, 1888 women were included. VTE incidence densities on and off hormonal therapy were 3.7%/year and 4.7%/year (adjusted HR, 0.56; 95% confidence interval [CI], 0.23-1.39), respectively, and were 3.7%/year and 3.8%/year, respectively, for estrogen-containing and progestin-only therapy. The adjusted HR for all abnormal uterine bleeding (on vs off hormonal therapy) was 1.02 (95% CI, 0.66-1.57). Abnormal uterine bleeding occurred more frequently with rivaroxaban than with enoxaparin/VKA (HR, 2.13; 95% CI, 1.57-2.89). Hormonal therapy was not associated with an increased risk of recurrent VTE in women receiving therapeutic anticoagulation. The observed increased risk of abnormal uterine bleeding with rivaroxaban needs further exploration.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Less menorrhagia for women with VTE.Blood. 2016 Mar 17;127(11):1378-9. doi: 10.1182/blood-2016-01-692053. Blood. 2016. PMID: 26989185
References
-
- Hall JG, Pauli RM, Wilson KM. Maternal and fetal sequelae of anticoagulation during pregnancy. Am J Med. 1980;68(1):122–140. - PubMed
-
- Bates SM, Greer IA, Hirsh J, Ginsberg JS. Use of antithrombotic agents during pregnancy: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):627S–644S. - PubMed
-
- Ginsberg JS, Hirsh J, Turner DC, Levine MN, Burrows R. Risks to the fetus of anticoagulant therapy during pregnancy. Thromb Haemost. 1989;61(2):197–203. - PubMed
-
- van der Hulle T, Kooiman J, den Exter PL, Dekkers OM, Klok FA, Huisman MV. Effectiveness and safety of novel oral anticoagulants as compared with vitamin K antagonists in the treatment of acute symptomatic venous thromboembolism: a systematic review and meta-analysis. J Thromb Haemost. 2014;12(3):320–328. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
