

Discrimination between Alzheimer's Disease and Late Onset Bipolar Disorder Using Multivariate Analysis
- PMID: 26696883
- PMCID: PMC4677464
- DOI: 10.3389/fnagi.2015.00231
Discrimination between Alzheimer's Disease and Late Onset Bipolar Disorder Using Multivariate Analysis
Abstract
Background: Late onset bipolar disorder (LOBD) is often difficult to distinguish from degenerative dementias, such as Alzheimer disease (AD), due to comorbidities and common cognitive symptoms. Moreover, LOBD prevalence in the elder population is not negligible and it is increasing. Both pathologies share pathophysiological neuroinflammation features. Improvements in differential diagnosis of LOBD and AD will help to select the best personalized treatment.
Objective: The aim of this study is to assess the relative significance of clinical observations, neuropsychological tests, and specific blood plasma biomarkers (inflammatory and neurotrophic), separately and combined, in the differential diagnosis of LOBD versus AD. It was carried out evaluating the accuracy achieved by classification-based computer-aided diagnosis (CAD) systems based on these variables.
Materials: A sample of healthy controls (HC) (n = 26), AD patients (n = 37), and LOBD patients (n = 32) was recruited at the Alava University Hospital. Clinical observations, neuropsychological tests, and plasma biomarkers were measured at recruitment time.
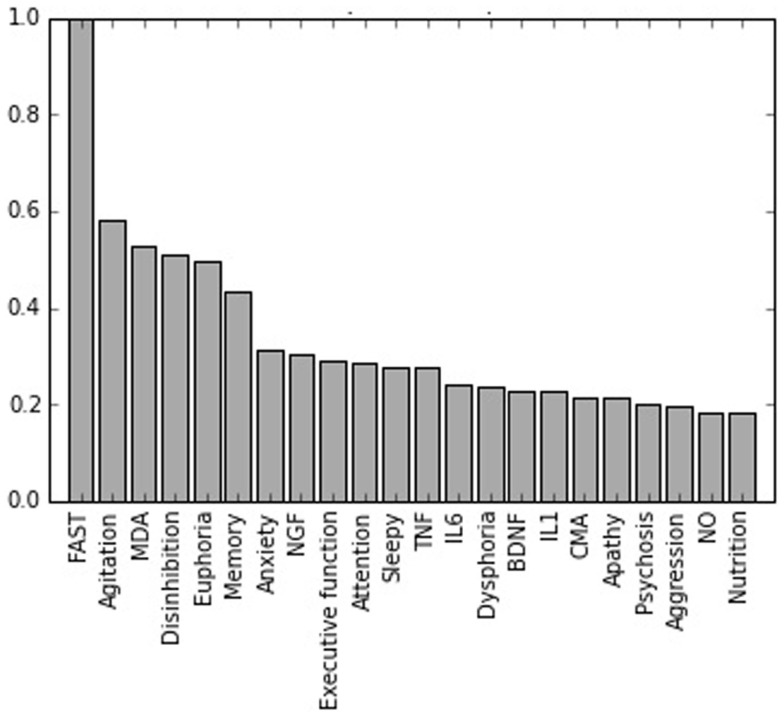
Methods: We applied multivariate machine learning classification methods to discriminate subjects from HC, AD, and LOBD populations in the study. We analyzed, for each classification contrast, feature sets combining clinical observations, neuropsychological measures, and biological markers, including inflammation biomarkers. Furthermore, we analyzed reduced feature sets containing variables with significative differences determined by a Welch's t-test. Furthermore, a battery of classifier architectures were applied, encompassing linear and non-linear Support Vector Machines (SVM), Random Forests (RF), Classification and regression trees (CART), and their performance was evaluated in a leave-one-out (LOO) cross-validation scheme. Post hoc analysis of Gini index in CART classifiers provided a measure of each variable importance.
Results: Welch's t-test found one biomarker (Malondialdehyde) with significative differences (p < 0.001) in LOBD vs. AD contrast. Classification results with the best features are as follows: discrimination of HC vs. AD patients reaches accuracy 97.21% and AUC 98.17%. Discrimination of LOBD vs. AD patients reaches accuracy 90.26% and AUC 89.57%. Discrimination of HC vs LOBD patients achieves accuracy 95.76% and AUC 88.46%.
Conclusion: It is feasible to build CAD systems for differential diagnosis of LOBD and AD on the basis of a reduced set of clinical variables. Clinical observations provide the greatest discrimination. Neuropsychological tests are improved by the addition of biomarkers, and both contribute significantly to improve the overall predictive performance.
Keywords: Alzheimer’s disease; and blood; biomarkers; clinical; computer-aided diagnosis; late onset bipolar disorder; neuropsychological; pharmacological.
Figures
Similar articles
-
White Matter Tract Integrity in Alzheimer's Disease vs. Late Onset Bipolar Disorder and Its Correlation with Systemic Inflammation and Oxidative Stress Biomarkers.Front Aging Neurosci. 2017 Jun 16;9:179. doi: 10.3389/fnagi.2017.00179. eCollection 2017. Front Aging Neurosci. 2017. PMID: 28670271 Free PMC article.
-
Eigenanatomy on Fractional Anisotropy Imaging Provides White Matter Anatomical Features Discriminating Between Alzheimer's Disease and Late Onset Bipolar Disorder.Curr Alzheimer Res. 2016;13(5):557-65. doi: 10.2174/1567205013666151116125349. Curr Alzheimer Res. 2016. PMID: 26567744
-
Analysis of structural brain MRI and multi-parameter classification for Alzheimer's disease.Biomed Tech (Berl). 2018 Jul 26;63(4):427-437. doi: 10.1515/bmt-2016-0239. Biomed Tech (Berl). 2018. PMID: 28622141
-
[Validation of the Short Cognitive Battery (B2C). Value in screening for Alzheimer's disease and depressive disorders in psychiatric practice].Encephale. 2003 May-Jun;29(3 Pt 1):266-72. Encephale. 2003. PMID: 12876552 French.
-
A Comprehensive Review of Computer-Aided Diagnosis of Major Mental and Neurological Disorders and Suicide: A Biostatistical Perspective on Data Mining.Diagnostics (Basel). 2021 Feb 25;11(3):393. doi: 10.3390/diagnostics11030393. Diagnostics (Basel). 2021. PMID: 33669114 Free PMC article. Review.
Cited by
-
Schistosoma mansoni reinfection: Analysis of risk factors by classification and regression tree (CART) modeling.PLoS One. 2017 Aug 16;12(8):e0182197. doi: 10.1371/journal.pone.0182197. eCollection 2017. PLoS One. 2017. PMID: 28813451 Free PMC article.
-
An Imaging and Blood Biomarkers Open Dataset on Alzheimer's Disease vs. Late Onset Bipolar Disorder.Front Aging Neurosci. 2020 Oct 29;12:583212. doi: 10.3389/fnagi.2020.583212. eCollection 2020. Front Aging Neurosci. 2020. PMID: 33192477 Free PMC article. No abstract available.
-
White Matter Tract Integrity in Alzheimer's Disease vs. Late Onset Bipolar Disorder and Its Correlation with Systemic Inflammation and Oxidative Stress Biomarkers.Front Aging Neurosci. 2017 Jun 16;9:179. doi: 10.3389/fnagi.2017.00179. eCollection 2017. Front Aging Neurosci. 2017. PMID: 28670271 Free PMC article.
-
In Silico Prediction of Gamma-Aminobutyric Acid Type-A Receptors Using Novel Machine-Learning-Based SVM and GBDT Approaches.Biomed Res Int. 2016;2016:2375268. doi: 10.1155/2016/2375268. Epub 2016 Aug 8. Biomed Res Int. 2016. PMID: 27579307 Free PMC article.
-
Machine learning algorithm performance evaluation in structural magnetic resonance imaging-based classification of pediatric bipolar disorders type I patients.Front Comput Neurosci. 2022 Aug 23;16:915477. doi: 10.3389/fncom.2022.915477. eCollection 2022. Front Comput Neurosci. 2022. PMID: 36082304 Free PMC article.
References
-
- Barandiaran I., Paloc C., Graña M. (2010). Real-time optical markerles tracking for augmented reality applications. J. Real Time Image Process. 5, 129–138.10.1007/s11554-009-0140-2 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous