

Thirty days post-operative mortality after surgery for colorectal cancer: a descriptive study
- PMID: 26697192
- PMCID: PMC4671843
- DOI: 10.3978/j.issn.2078-6891.2015.079
Thirty days post-operative mortality after surgery for colorectal cancer: a descriptive study
Abstract
Background: The goal of surgery for colorectal cancer is cure. Unfortunately post-operative mortality occurs. This study aims to identify co-morbidity and causes of mortality in the post-operative period in relation to direct technical complications of surgery.
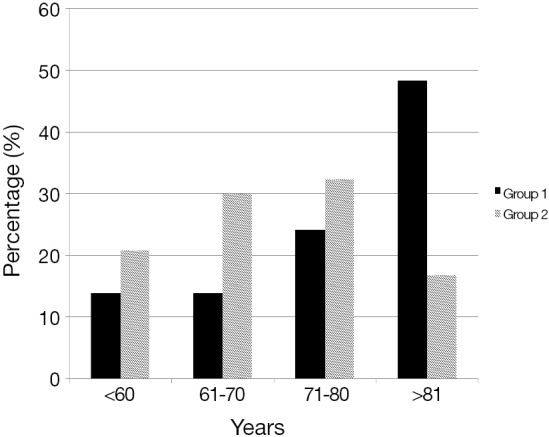
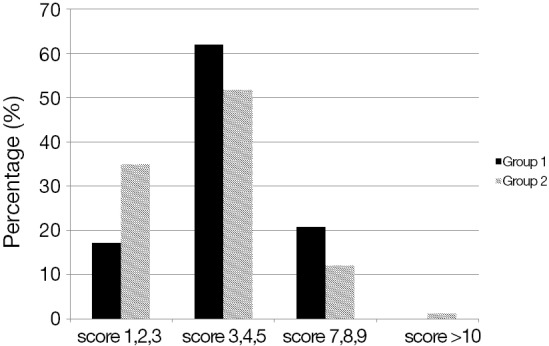
Methods: All consecutive patients who underwent surgery for colorectal cancer were included. Co-morbidity was determined via the Charlson co-morbidity score. The post-operative course was studied and cause of death within 30 days was determined. Patients were divided in two groups: group 1 died within 30 days after surgery and group 2 survived for longer than 30 days.
Results: Twenty three out of 333 patients (6.9%) with colon cancer and 6 out of 112 (5.3%) with rectal cancer died in the post-operative period. Patients in group 1 were significantly older than patients in group 2 (P<0.001). Patients in group 1 with colon cancer also significantly had more often a higher stage of cancer (P=0.03). The Charlson co-morbidity score for patients with colon cancer in group 1 was mean 5.17 (SD 1.57, range, 1-8), and for rectal cancer mean 4.83 (SD 2.32, range, 2-7). There was no difference in Charlson co-morbidity score when patients from groups 1 and 2 were compared. In group 1, 13 (44%) died as a direct consequence of technical surgical complications. Sixteen patients died due to complications because of pre-existing co-morbidity.
Conclusions: Post-operative mortality very often is the direct result of pre-existing co-morbidity and not always the direct result of the surgical procedure.
Keywords: Charlson score; Colorectal cancer; anastomotic leakage; bleeding; post-operative mortality.
Conflict of interest statement
Figures
References
-
- Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108. - PubMed
-
- Rim SH, Seeff L, Ahmed F, et al. Colorectal cancer incidence in the United States, 1999-2004: an updated analysis of data from the National Program of Cancer Registries and the Surveillance, Epidemiology, and End Results Program. Cancer 2009;115:1967-76. - PubMed
-
- Dutch Cancer registration. Available online: www.cijfersoverkanker.nl
-
- Integral Cancer Institute Amsterdam. Available online: www.ika.nl
LinkOut - more resources
Full Text Sources