

Evaluation of a systematic approach to weaning of tracheotomized neurological patients: an early interrupted randomized controlled trial
- PMID: 26698596
- PMCID: PMC4689720
- DOI: 10.1186/s13613-015-0098-0
Evaluation of a systematic approach to weaning of tracheotomized neurological patients: an early interrupted randomized controlled trial
Abstract
Background: While a systematic approach to weaning reduces the rate of extubation failure in intubated brain-injured patients, no data are available on the weaning outcome of these patients after tracheotomy. We aimed to assess whether a systematic approach to disconnect tracheotomized neurological and neurosurgical patients off the ventilator (intervention) is superior to the sole physician's judgment (control). Based on previous work in intubated patients, we hypothesized a reduction of the rate of failure within 48 h from 15 to 5 %. Secondary endpoints were duration of mechanical ventilation, ICU length of stay and mortality.
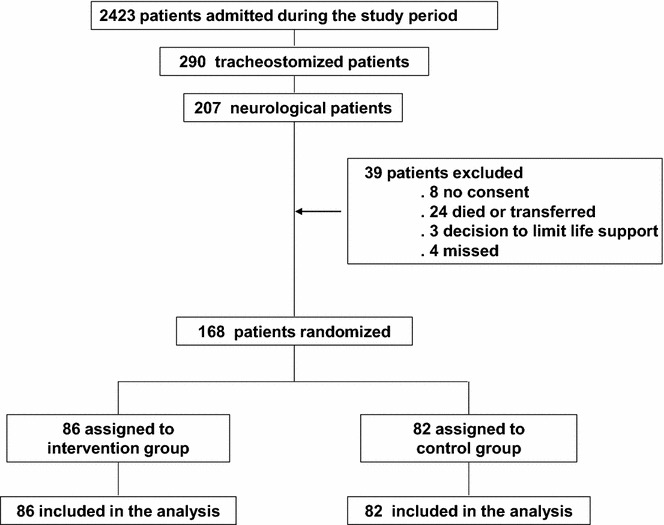
Methods: We designed a single center randomized controlled study. Since no data are available on tracheotomized patients, we based our a priori power analysis on results derived from intubated patients and calculated an overall sample size of 280 patients.
Results: After inclusion of 168 consecutive patients, the trial was interrupted because the attending physicians judged the observed rate of reconnection to be much greater than expected. The overall rate of failure was 29 %, confirming the physicians' judgment. Twenty-one patients (24 %) in the intervention group and 27 (33 %) controls were reconnected to the ventilator within 48 h (p = 0.222). The main reasons for failure were respiratory distress (80 and 88 % in the treatment and control group, respectively), hemodynamic impairment (15 and 4 % in the treatment and control group, respectively), neurological deterioration (4 % in the control group only). The duration of mechanical ventilation was of 412 ± 202 h and 402 ± 189 h, in the control and intervention group, respectively. ICU length of stay was on average of 23 days for both groups. ICU mortality was 6 % in the control and 2 % in the intervention group without significant differences.
Conclusion: We found no difference between the two groups under evaluation, with a rate of failure much higher than expected. Consequent to the early interruption, our study results to be underpowered. Based on the results of the present study, a further trial should overall enroll 790 patients.
Trial registration: ACTRN12612000372886.
Keywords: Brain-injured patients; Tracheotomy; Weaning.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
