

Diagnostic performance of FDG-PET/MRI and WB-DW-MRI in the evaluation of lymphoma: a prospective comparison to standard FDG-PET/CT
- PMID: 26699124
- PMCID: PMC4690292
- DOI: 10.1186/s12885-015-2009-z
Diagnostic performance of FDG-PET/MRI and WB-DW-MRI in the evaluation of lymphoma: a prospective comparison to standard FDG-PET/CT
Abstract
Background: Use of FDG-PET/CT for staging and restaging of lymphoma patients is widely incorporated into current practice guidelines. Our aim was to prospectively evaluate the diagnostic performance of FDG-PET/MRI and WB-DW-MRI compared with FDG-FDG-PET/CT using a tri-modality PET/CT-MRI system.
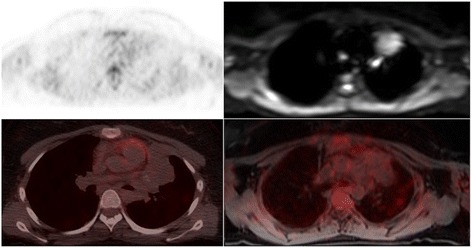
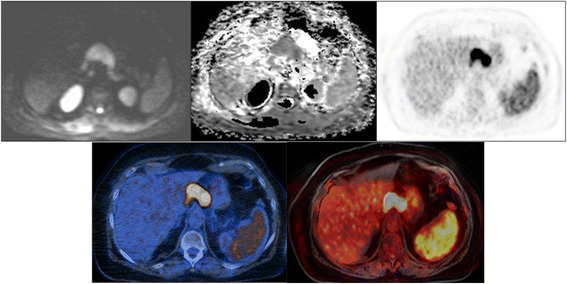
Methods: From 04/12 to 01/14, a total of 82 FDG-PET/CT examinations including an additional scientific MRI on a tri-modality setup were performed in 61 patients. FDG-PET/CT, FDG-PET/MRI, and WB-DW-MRI were independently analyzed. A lesion with a mean ADC below a threshold of 1.2 × 10(-3) mm(2)/s was defined as positive for restricted diffusion. FDG-PET/CT and FDG-PET/MRI were evaluated for the detection of lesions corresponding to lymphoma manifestations according to the German Hodgkin Study Group. Imaging findings were validated by biopsy (n = 21), by follow-up imaging comprising CT, FDG-PET/CT, and/or FDG-PET/MRI (n = 32), or clinically (n = 25) (mean follow-up: 9.1 months).
Results: FDG-PET/MRI and FDG-PET/CT accurately detected 188 lesions in 27 patients. Another 54 examinations in 35 patients were negative. WB-DW-MRI detected 524 lesions, of which 125 (66.5% of the aforementioned 188 lesions) were true positive. Among the 188 lesions positive for lymphoma, FDG-PET/MRI detected all 170 instances of nodal disease and also all 18 extranodal lymphoma manifestations; by comparison, WB-DW-MRI characterized 115 (67.6%) and 10 (55.6%) lesions as positive for nodal and extranodal disease, respectively. FDG-PET/MRI was superior to WB-DW-MRI in detecting lymphoma manifestations in patients included for staging (113 vs. 73), for restaging (75 vs. 52), for evaluation of high- (127 vs. 81) and low-grade lymphomas (61 vs. 46), and for definition of Ann Arbor stage (WB-DW-MRI resulted in upstaging in 60 cases, including 45 patients free of disease, and downstaging in 4).
Conclusion: Our results indicate that FDG-PET/CT and FDG-PET/MRI probably have a similar performance in the clinical work-up of lymphomas. The performance of WB-DW-MRI was generally inferior to that of both FDG-PET-based methods but the technique might be used in specific scenarios, e.g., in low-grade lymphomas and during surveillance.
Figures
References
-
- Lin C, Luciani A, Itti E, El-Gnaoui T, Vignaud A, Beaussart P, et al. Whole-body diffusion-weighted magnetic resonance imaging with apparent diffusion coefficient mapping for staging patients with diffuse large B-cell lymphoma. Eur Radiol. 2010;20:2027–38. doi: 10.1007/s00330-010-1758-y. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
