

Prediction of All-Cause Mortality Based on the Direct Measurement of Intrathoracic Impedance
- PMID: 26699393
- PMCID: PMC4692195
- DOI: 10.1161/CIRCHEARTFAILURE.115.002543
Prediction of All-Cause Mortality Based on the Direct Measurement of Intrathoracic Impedance
Abstract
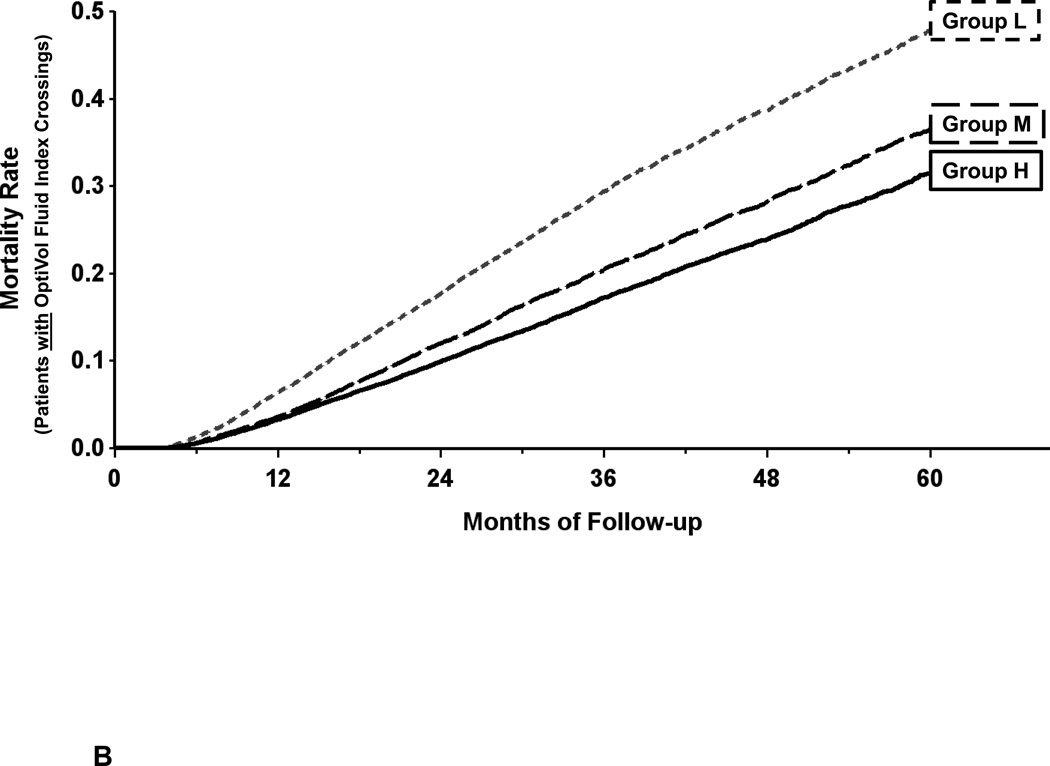
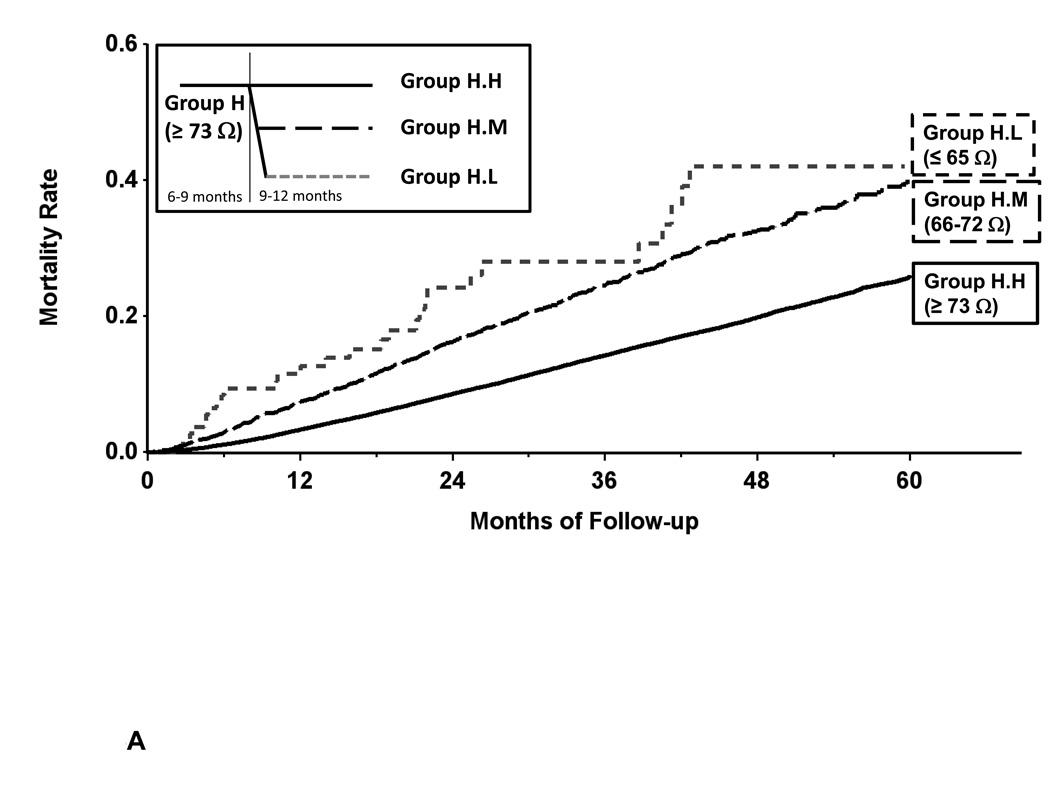
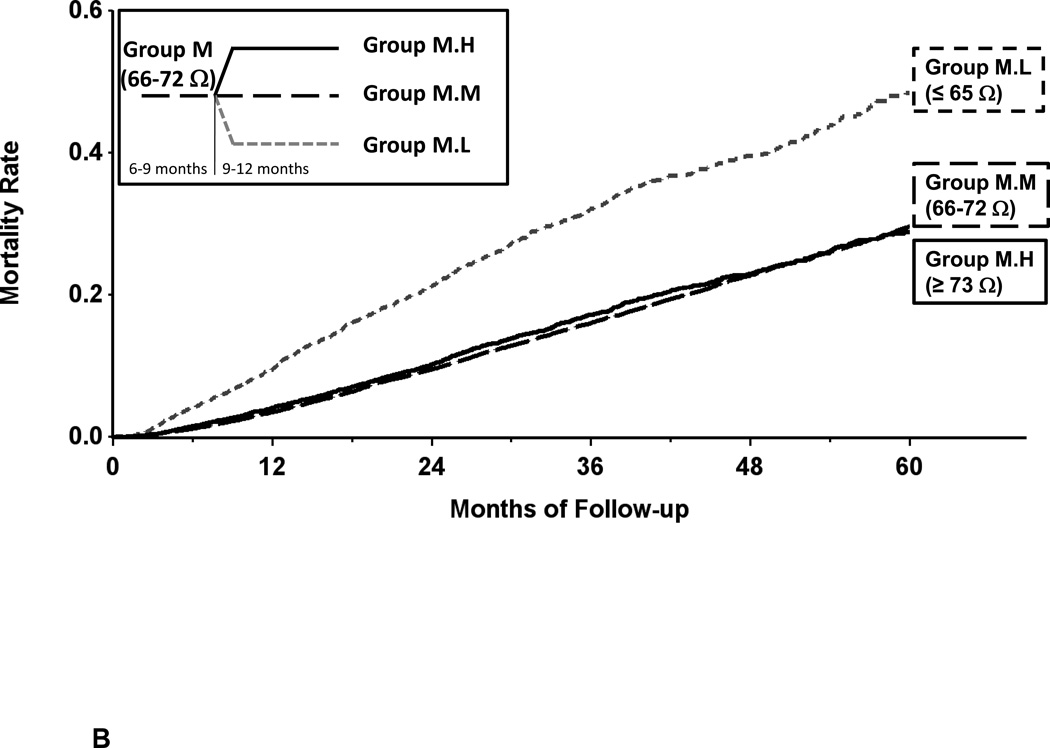
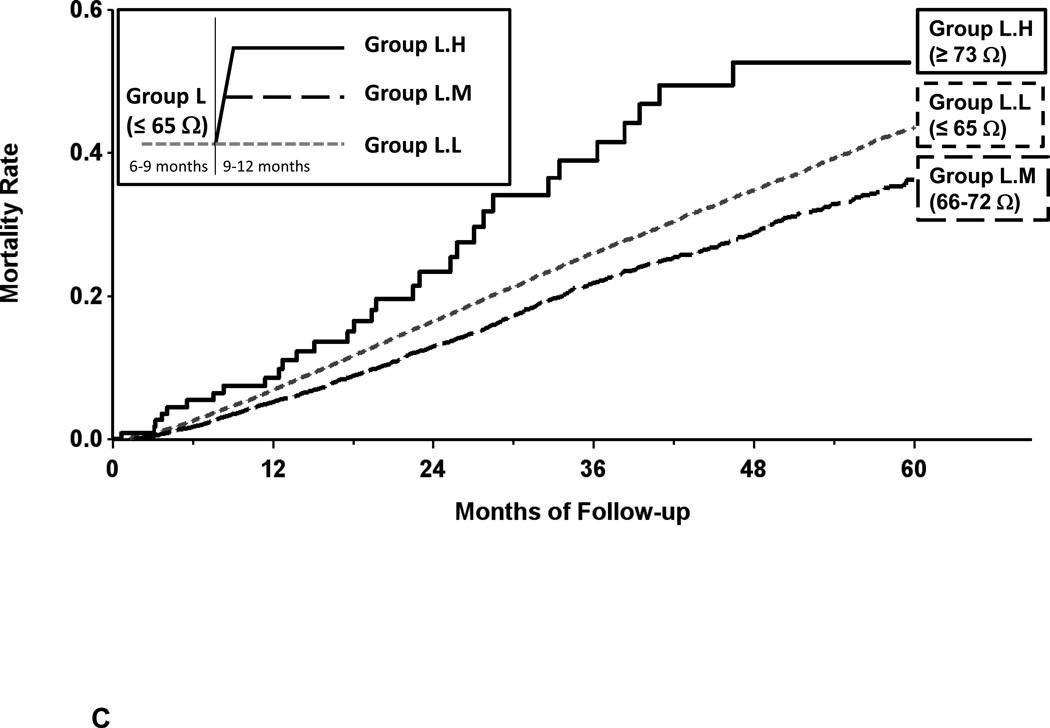
Background: Intrathoracic impedance-derived OptiVol fluid index calculated using implanted devices has been shown to predict mortality; direct measurements of impedance have not been examined. We hypothesized that baseline measured impedance predicts all-cause mortality; changes in measured impedance result in a change in the predicted mortality; and the prognostic value of measured impedance is additive to the calculated OptiVol fluid index.
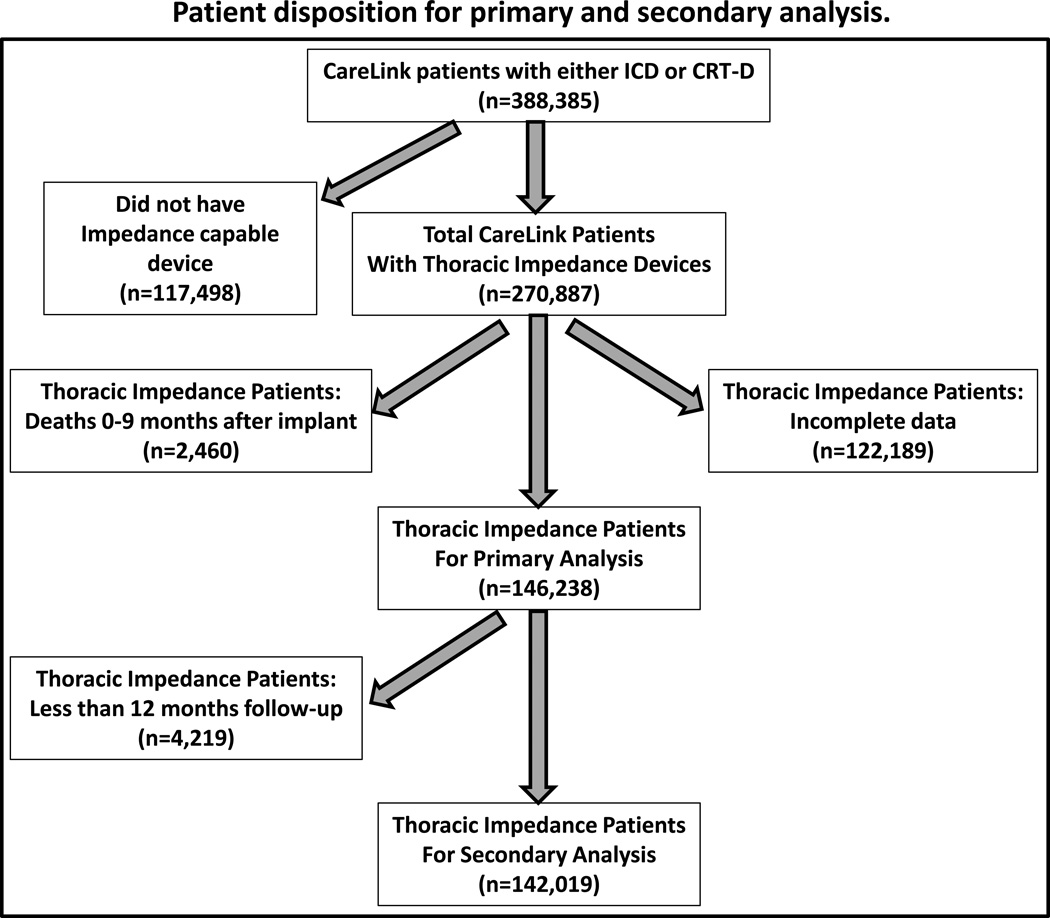
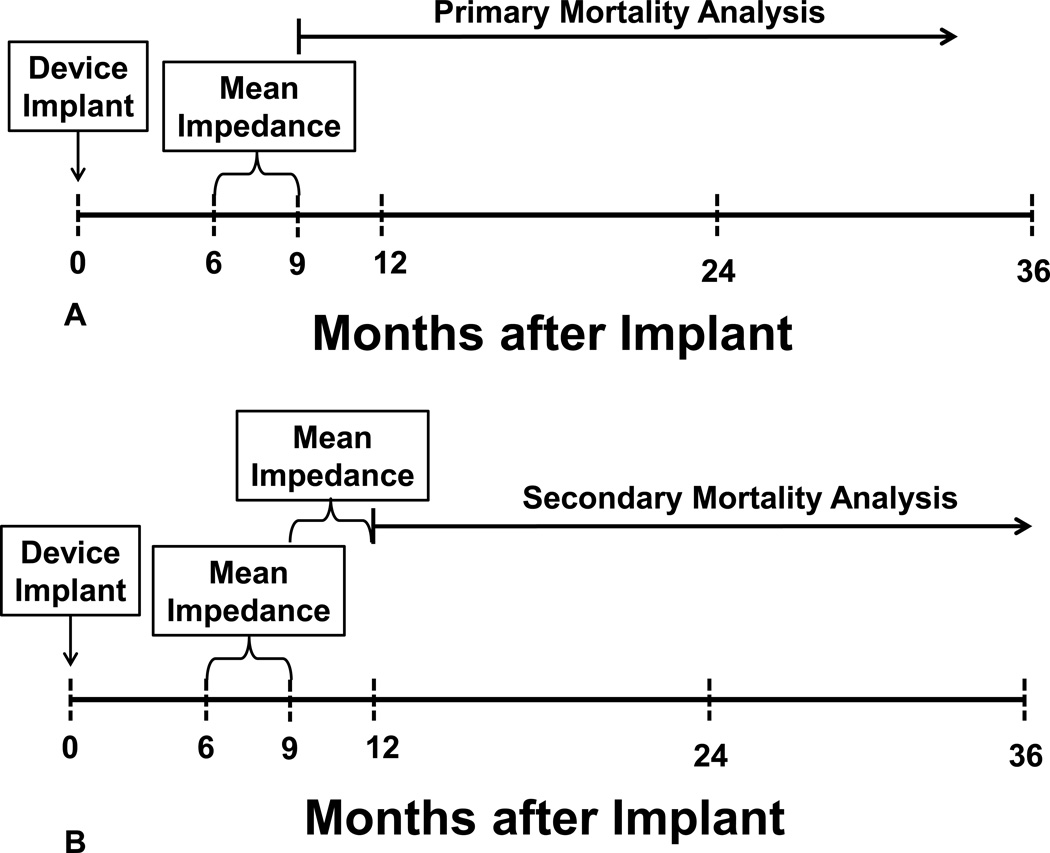
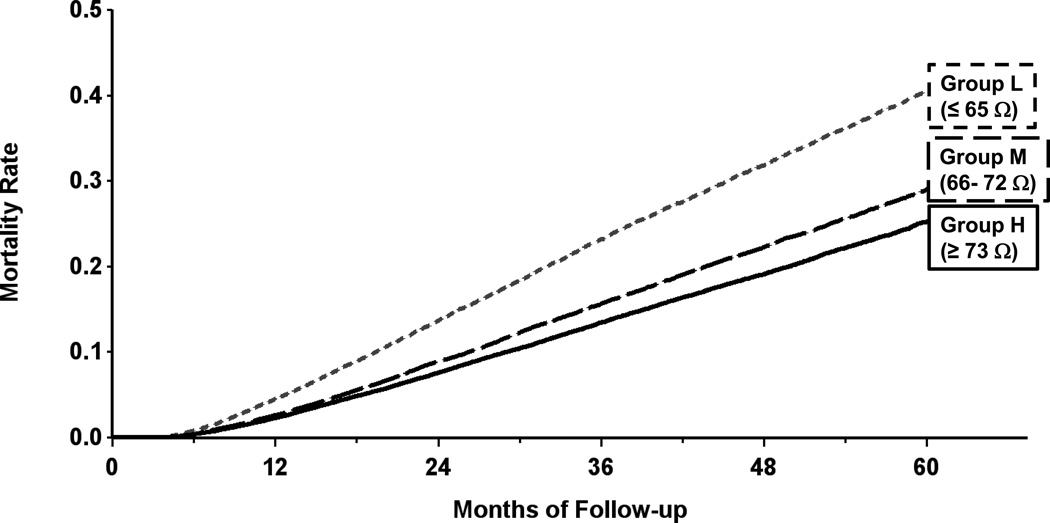
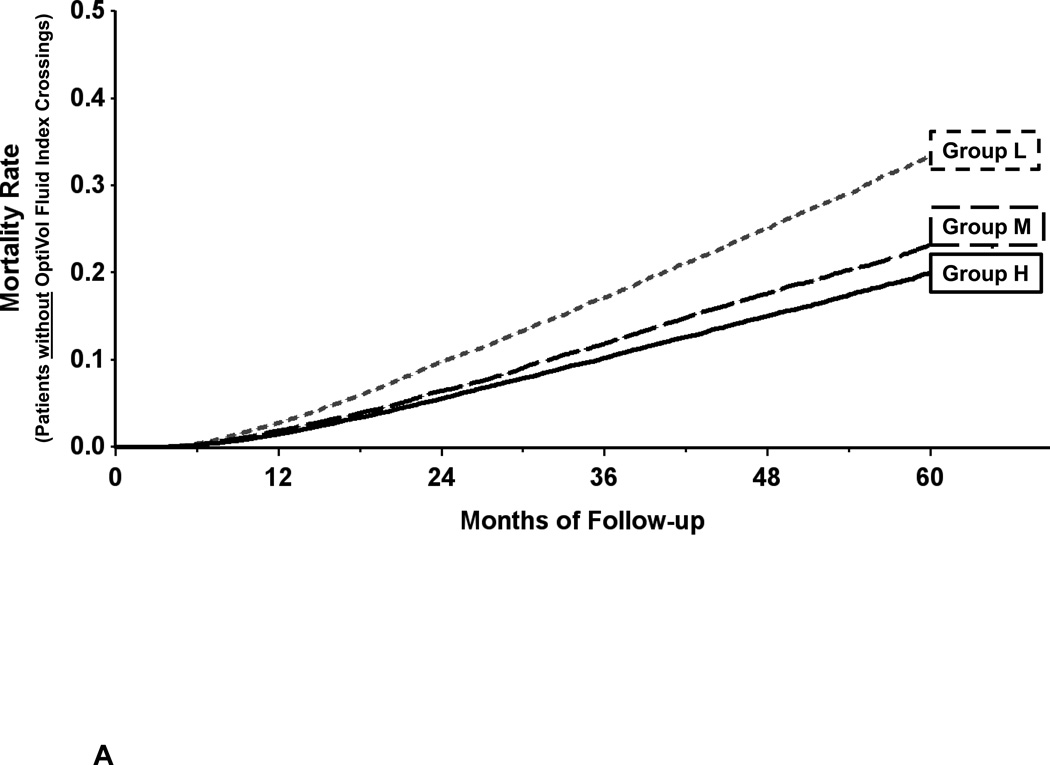
Methods and results: A retrospective analysis of 146,238 patients within the Medtronic CareLink database with implanted devices was performed. Baseline measured impedance was determined using daily values averaged from month 6 to 9 after implant and were used to divide patients into tertiles: group L = low impedance, ≤ 65 ohms; group M = medium impedance, 66 to 72 ohms; group H = high impedance, ≥ 73 ohms. Change in measured impedance was determined from values averaged from month 9 to 12 post implant compared with the 6- to 9-month values. OptiVol fluid index was calculated using published methods. All-cause mortality was assessed beginning 9 months post implant; changes in mortality was assessed beginning 12 months post implant. Baseline measured impedance predicted all-cause mortality; 5-year mortality for group L was 41%, M was 29%, and H was 25%, P < 0.001 among all groups. Changes in measured impedance resulted in a change in the predicted mortality; the prognostic value of measured impedance was additive to the OptiVol fluid index.
Conclusions: Direct measurements of intrathoracic impedance using an implanted device can be used to stratify patients at varying mortality risk.
Keywords: all-cause mortality; heart failure; impedance; risk.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
Assessing Impedance in Heart Failure: From Device Diagnostics to Population Health Opportunities?Circ Heart Fail. 2016 Jan;9(1):e002761. doi: 10.1161/CIRCHEARTFAILURE.115.002761. Epub 2015 Dec 23. Circ Heart Fail. 2016. PMID: 26699395 No abstract available.
References
-
- Yu CM, Wang L, Chau E, Chan RH, Kong SL, Tang MO, Christensen J, Stadler RW, Lau CP. Intrathoracic impedance monitoring in patients with heart failure: correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation. 2005;112:841–848. - PubMed
-
- Conraads VM, Tavazzi L, Santini M, Oliva F, Gerritse B, Yu CM, Cowie MR. Sensitivity and positive predictive value of implantable intrathoracic impedance monitoring as a predictor of heart failure hospitalizations: the SENSE-HF trial. European heart journal. 2011;32:2266–2273. - PubMed
-
- Small RS, Wickemeyer W, Germany R, Hoppe B, Andrulli J, Brady PA, Labeau M, Koehler J, Sarkar S, Hettrick DA, Tang WH. Changes in intrathoracic impedance are associated with subsequent risk of hospitalizations for acute decompensated heart failure: clinical utility of implanted device monitoring without a patient alert. J Card Fail. 2009;15:475–481. - PubMed
-
- Wang L. Fundamentals of intrathoracic impedance monitoring in heart failure. Am J Cardiol. 2007;99:3G–10G. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
