

Mapping tissue inhomogeneity in acute myocarditis: a novel analytical approach to quantitative myocardial edema imaging by T2-mapping
- PMID: 26700020
- PMCID: PMC4690253
- DOI: 10.1186/s12968-015-0217-y
Mapping tissue inhomogeneity in acute myocarditis: a novel analytical approach to quantitative myocardial edema imaging by T2-mapping
Abstract
Background: The purpose of the present study was to investigate the diagnostic value of T2-mapping in acute myocarditis (ACM) and to define cut-off values for edema detection.
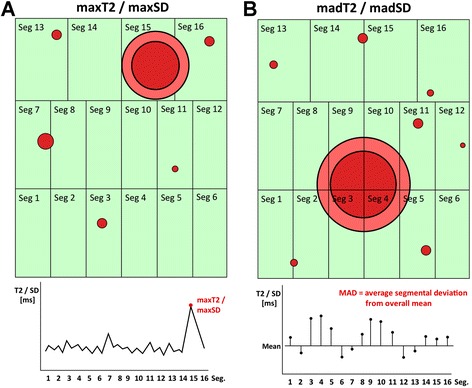
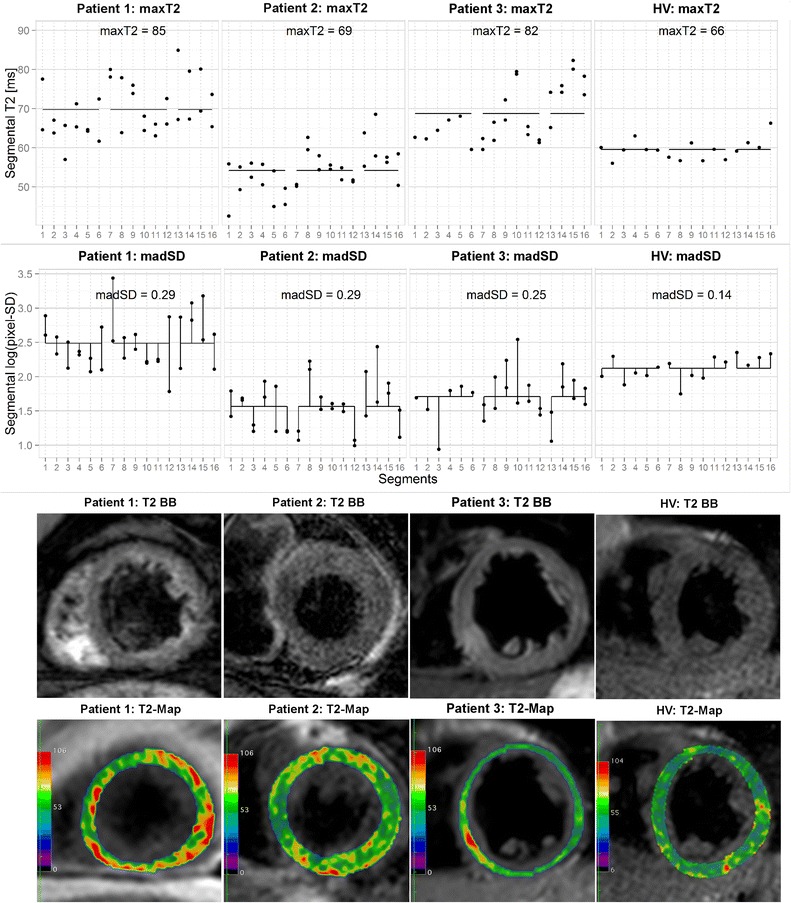
Methods: Cardiovascular magnetic resonance (CMR) data of 31 patients with ACM were retrospectively analyzed. 30 healthy volunteers (HV) served as a control. Additionally to the routine CMR protocol, T2-mapping data were acquired at 1.5 T using a breathhold Gradient-Spin-Echo T2-mapping sequence in six short axis slices. T2-maps were segmented according to the 16-segments AHA-model and segmental T2 values as well as the segmental pixel-standard deviation (SD) were analyzed.
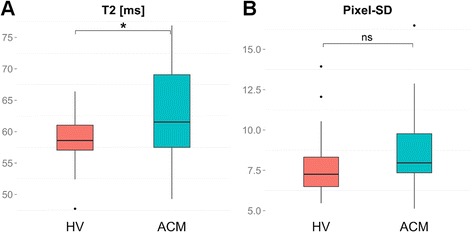
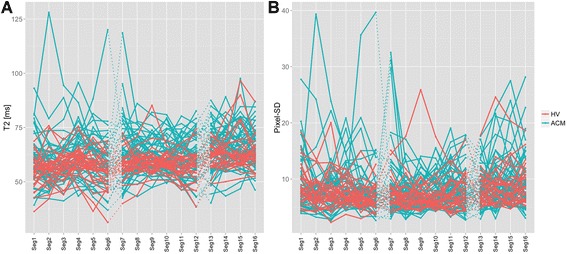
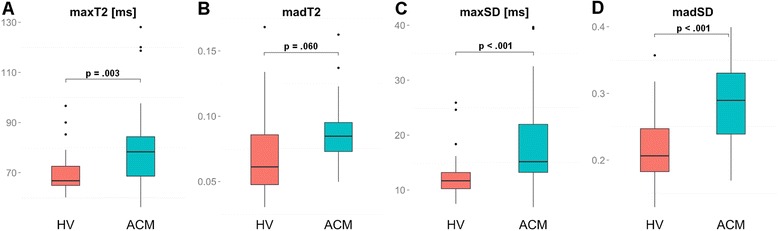
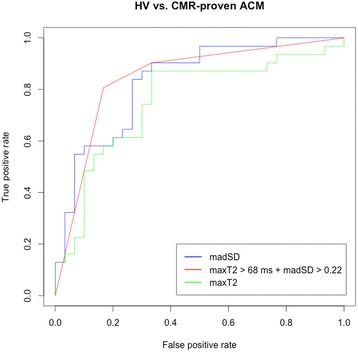
Results: Mean differences of global myocardial T2 or pixel-SD between HV and ACM patients were only small, lying in the normal range of HV. In contrast, variation of segmental T2 values and pixel-SD was much larger in ACM patients compared to HV. In random forests and multiple logistic regression analyses, the combination of the highest segmental T2 value within each patient (maxT2) and the mean absolute deviation (MAD) of log-transformed pixel-SD (madSD) over all 16 segments within each patient proved to be the best discriminators between HV and ACM patients with an AUC of 0.85 in ROC-analysis. In classification trees, a combined cut-off of 0.22 for madSD and of 68 ms for maxT2 resulted in 83% specificity and 81% sensitivity for detection of ACM.
Conclusions: The proposed cut-off values for maxT2 and madSD in the setting of ACM allow edema detection with high sensitivity and specificity and therefore have the potential to overcome the hurdles of T2-mapping for its integration into clinical routine.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
