

Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a Phase III randomized controlled trial
- PMID: 26701110
- PMCID: PMC4690334
- DOI: 10.1186/s12933-015-0314-0
Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a Phase III randomized controlled trial
Abstract
Background: To investigate the long-term efficacy and safety of empagliflozin monotherapy compared with placebo and sitagliptin in drug-naïve patients with type 2 diabetes mellitus.
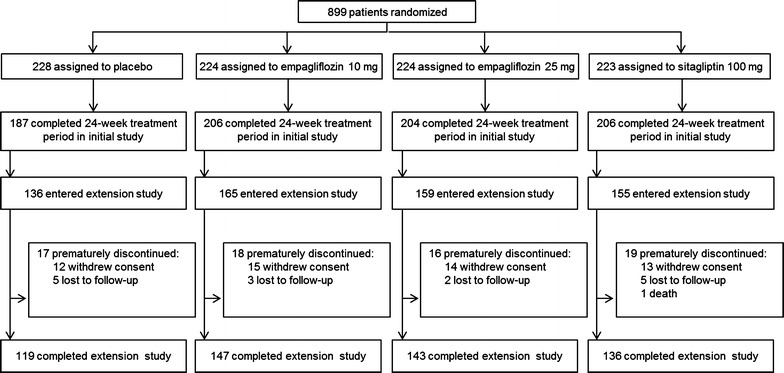
Methods: Of 899 patients randomized to receive empagliflozin 10 mg, empagliflozin 25 mg, placebo, or sitagliptin 100 mg once daily for 24 weeks, 615 continued in a double-blind extension trial for ≥52 weeks. Exploratory endpoints included changes from baseline in HbA1c, weight and blood pressure at week 76.
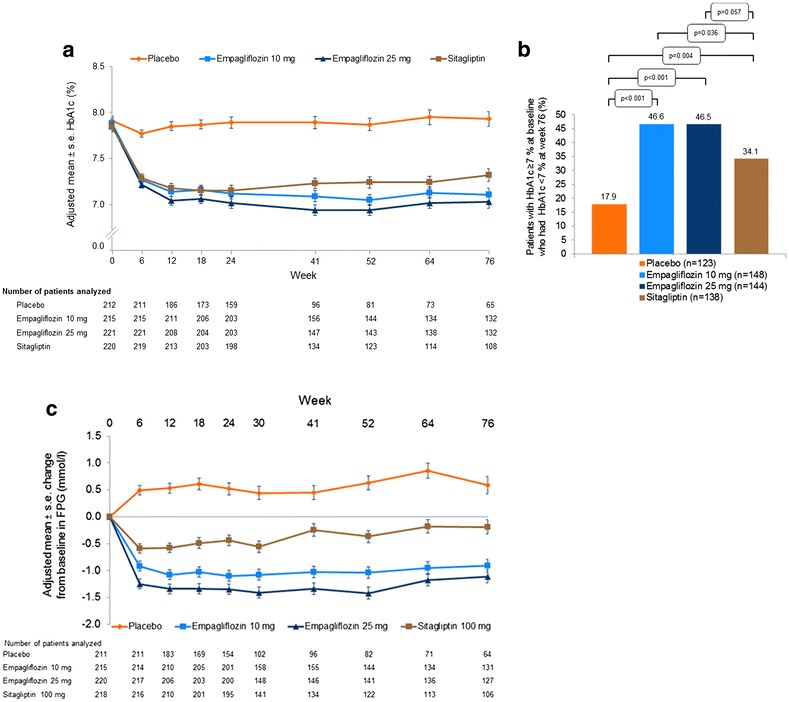
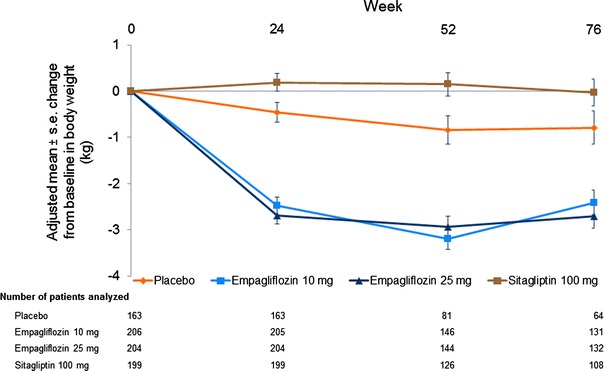
Results: Compared with placebo, adjusted mean changes from baseline in HbA1c at week 76 were -0.78 % (95 % CI -0.94, -0.63; p < 0.001) and -0.89 % (95 % CI -1.04, -0.73; p < 0.001) for empagliflozin 10 mg and 25 mg, respectively. Compared with placebo, adjusted mean changes from baseline in weight at week 76 were -1.8 kg (95 % CI -2.4, -1.3; p < 0.001) and -2.0 kg (95 % CI -2.6, -1.5; p < 0.001) for empagliflozin 10 mg and 25 mg, respectively. Empagliflozin led to reductions in systolic blood pressure (SBP) compared with placebo in the primary analysis but not in sensitivity analyses. Compared with sitagliptin, empagliflozin 25 mg reduced HbA1c and both empagliflozin doses reduced weight and SBP. Adverse events (AEs) were reported in 76.8, 78.0, 76.4 and 72.2 % of patients on empagliflozin 10 mg, empagliflozin 25 mg, placebo and sitagliptin, respectively. Confirmed hypoglycaemic AEs (glucose ≤3.9 mmol/l and/or requiring assistance) were reported in two patients (0.9 %) per treatment group.
Conclusions: Empagliflozin monotherapy for ≥76 weeks was well tolerated and led to sustained reductions in HbA1c and weight compared with placebo.
Trial registration: clinicaltrials.gov NCT01289990.
Figures
References
-
- Baker WL, Smyth LR, Riche DM, Bourret EM, Chamberlin KW, White WB. Effects of sodium-glucose co-transporter 2 inhibitors on blood pressure: a systematic review and meta-analysis. J Am Soc Hypertens. 2014;8(262–75):e9. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
