

Neurologist ambulatory care, health care utilization, and costs in a large commercial dataset
- PMID: 26701378
- PMCID: PMC4776087
- DOI: 10.1212/WNL.0000000000002276
Neurologist ambulatory care, health care utilization, and costs in a large commercial dataset
Abstract
Objective: To determine the value of neurologist ambulatory care in chronic neurologic diseases in a large administrative claims dataset detailing costs, adverse events, and health care utilization.
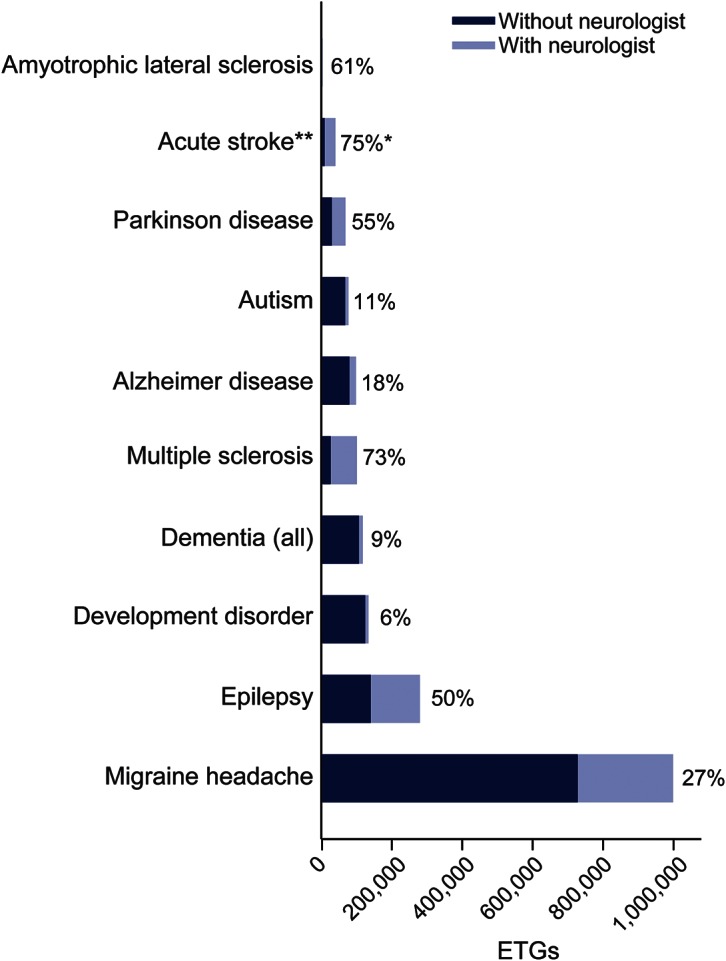
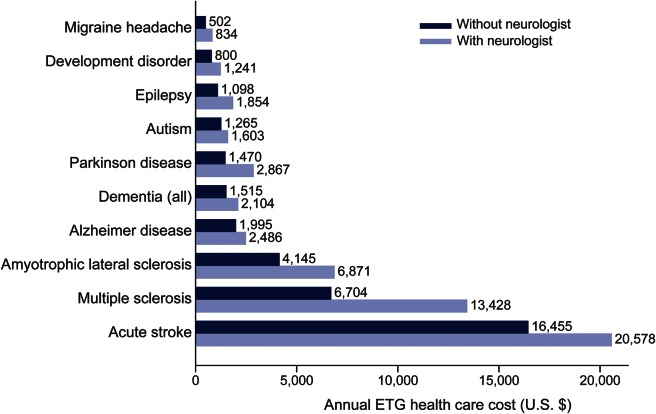
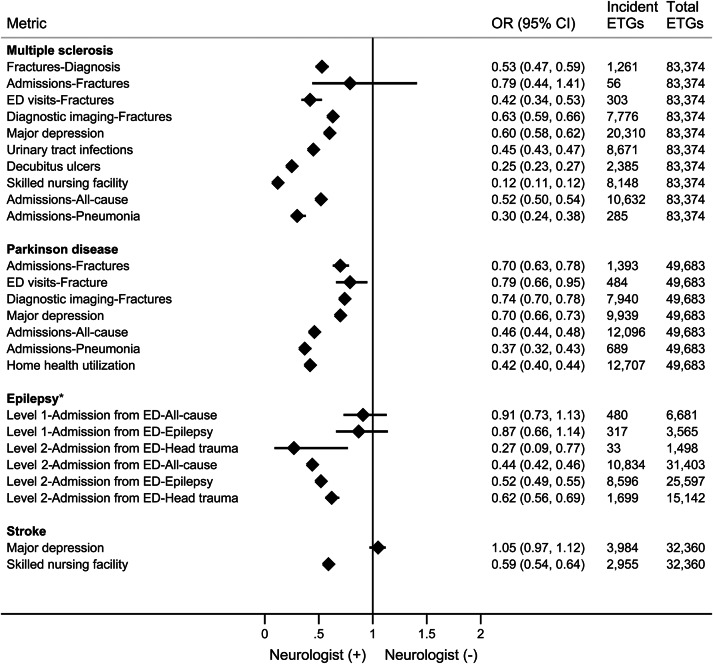
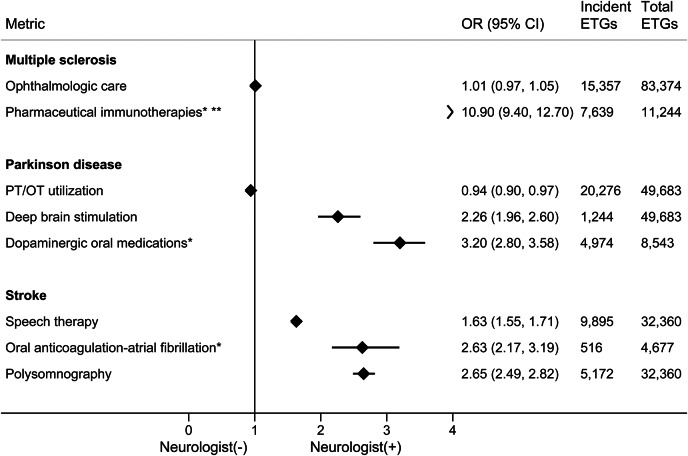
Methods: The Optum proprietary claims dataset (2010-2012) was examined to describe direct health care costs, as well as specific outcome metrics for a large population of persons with chronic neurologic illnesses. In phase I of the study, we detail neurologist involvement and differences in annualized allowed third--party payments within episode treatment groups (ETGs) for 10 neurologic illnesses. For phase II, we examined health care utilization for ETGs of epilepsy, Parkinson disease (PD), stroke, and multiple sclerosis (MS) with and without neurologist involvement. Reported outcomes were unadjusted differences and odds ratios between treatment groups.
Results: For phase I, a total of 1,913,605 ETGs for 10 neurologic conditions were identified, 30.1% meeting criteria for neurologist involvement. All conditions had higher direct costs when neurologists were involved with care, ranging from a 25% increase for Alzheimer dementia to 100% more for MS care. In phase II, fractures, infections, emergent care, and inpatient admission were less with neurologist ambulatory care, while neurologist care was associated with greater utilization of disease-specific treatments (immunotherapies in MS anticoagulation in atrial fibrillation-associated stroke, deep brain stimulation and dopaminergic therapies in PD).
Conclusion: Neurologist involvement with care is associated with greater unadjusted allowed payments, but fewer adverse events and less acute care utilization.
© 2015 American Academy of Neurology.
Figures
Comment in
-
Measuring the value of neurology.Neurology. 2016 Jan 26;86(4):320-1. doi: 10.1212/WNL.0000000000002290. Epub 2015 Dec 23. Neurology. 2016. PMID: 26701377 No abstract available.
References
-
- Langel SJ. Crunching the really big numbers at CMS. Health Aff 2013;32:100–101. - PubMed
-
- Riley GF. Administrative and claims records as sources of health care cost data. Med Care 2009;47:S51–S55. - PubMed
-
- Serxner S, Alberti A, Weinberger S. Medical cost savings for participants and nonparticipants in health risk assessments, lifestyle management, disease management, depression management, and nurseline in a large financial services corporation. Am J Health Promot 2012;26:245–252. - PubMed
-
- Fallik D. For big data, big questions remain. Health Aff 2014;33:1111–1114. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical