

CKD Prevalence Varies across the European General Population
- PMID: 26701975
- PMCID: PMC4926978
- DOI: 10.1681/ASN.2015050542
CKD Prevalence Varies across the European General Population
Abstract
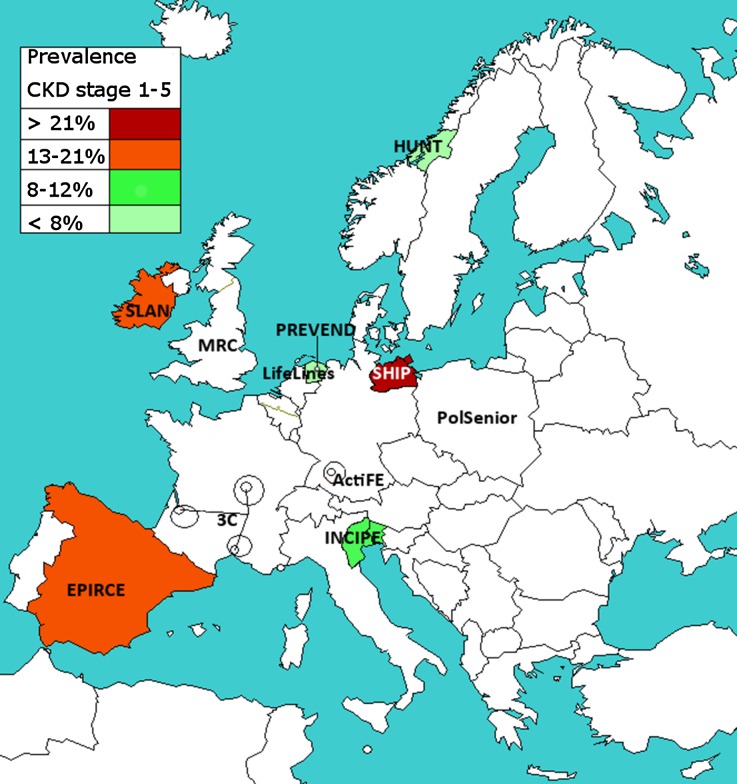
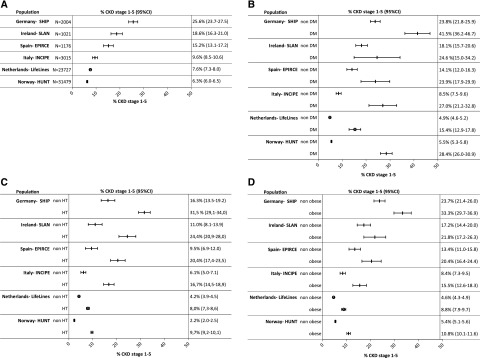
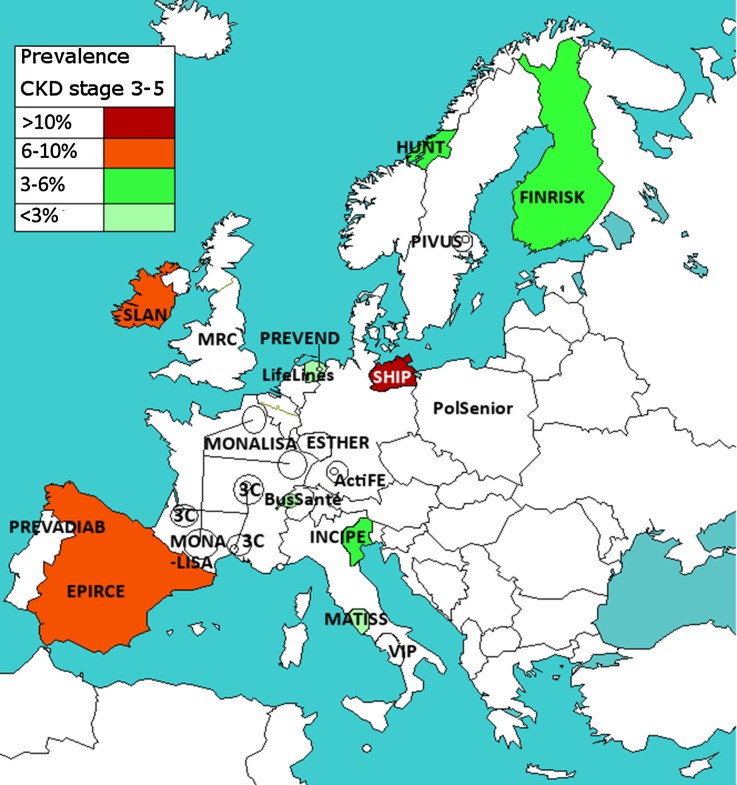
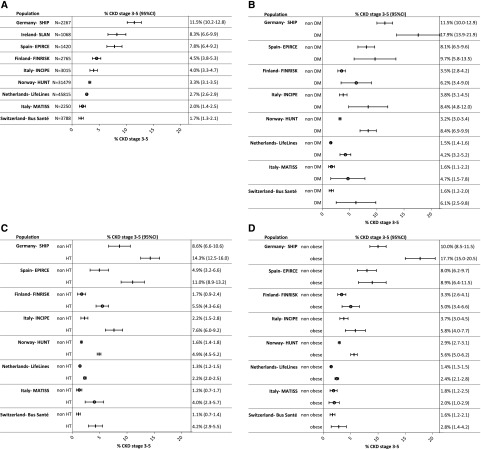
CKD prevalence estimation is central to CKD management and prevention planning at the population level. This study estimated CKD prevalence in the European adult general population and investigated international variation in CKD prevalence by age, sex, and presence of diabetes, hypertension, and obesity. We collected data from 19 general-population studies from 13 European countries. CKD stages 1-5 was defined as eGFR<60 ml/min per 1.73 m(2), as calculated by the CKD-Epidemiology Collaboration equation, or albuminuria >30 mg/g, and CKD stages 3-5 was defined as eGFR<60 ml/min per 1.73 m(2) CKD prevalence was age- and sex-standardized to the population of the 27 Member States of the European Union (EU27). We found considerable differences in both CKD stages 1-5 and CKD stages 3-5 prevalence across European study populations. The adjusted CKD stages 1-5 prevalence varied between 3.31% (95% confidence interval [95% CI], 3.30% to 3.33%) in Norway and 17.3% (95% CI, 16.5% to 18.1%) in northeast Germany. The adjusted CKD stages 3-5 prevalence varied between 1.0% (95% CI, 0.7% to 1.3%) in central Italy and 5.9% (95% CI, 5.2% to 6.6%) in northeast Germany. The variation in CKD prevalence stratified by diabetes, hypertension, and obesity status followed the same pattern as the overall prevalence. In conclusion, this large-scale attempt to carefully characterize CKD prevalence in Europe identified substantial variation in CKD prevalence that appears to be due to factors other than the prevalence of diabetes, hypertension, and obesity.
Keywords: chronic kidney disease; clinical epidemiology; creatinine.
Copyright © 2016 by the American Society of Nephrology.
Figures
Comment in
-
Unlocking the Value of Variation in CKD Prevalence.J Am Soc Nephrol. 2016 Jul;27(7):1874-7. doi: 10.1681/ASN.2015111280. Epub 2015 Dec 29. J Am Soc Nephrol. 2016. PMID: 26714870 Free PMC article. No abstract available.
References
-
- Kidney Disease. Improving Global Outcomes (KDIGO) CKD Work Group : KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl 3: 1–150, 2013
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP: Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet 382: 339–352, 2013 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- McCullough K, Sharma P, Ali T, Khan I, Smith WC, MacLeod A, Black C: Measuring the population burden of chronic kidney disease: a systematic literature review of the estimated prevalence of impaired kidney function. Nephrol Dial Transplant 27: 1812–1821, 2012 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
