

Early Left and Right Ventricular Response to Aortic Valve Replacement
- PMID: 26702865
- PMCID: PMC4945491
- DOI: 10.1213/ANE.0000000000001108
Early Left and Right Ventricular Response to Aortic Valve Replacement
Abstract
Background: The immediate effect of aortic valve replacement (AVR) for aortic stenosis on perioperative myocardial function is unclear. Left ventricular (LV) function may be impaired by cardioplegia-induced myocardial arrest and ischemia-reperfusion injury, especially in patients with LV hypertrophy. Alternatively, LV function may improve when afterload is reduced after AVR. The right ventricle (RV), however, experiences cardioplegic arrest without benefiting from improved loading conditions. Which of these effects on myocardial function dominate in patients undergoing AVR for aortic stenosis has not been thoroughly explored. Our primary objective is thus to characterize the effect of intraoperative events on LV function during AVR using echocardiographic measures of myocardial deformation. Second, we evaluated RV function.
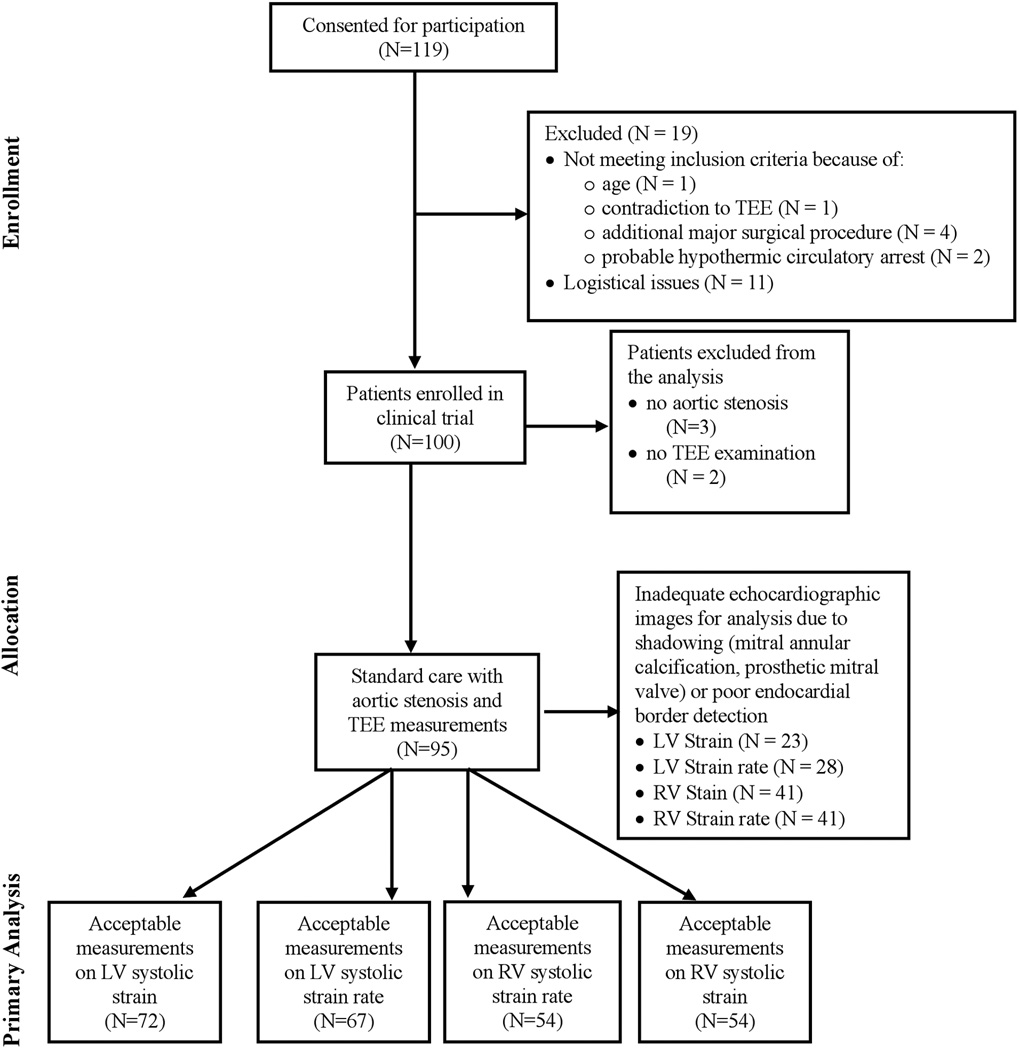
Methods: In this supplementary analysis of 100 patients enrolled in a clinical trial (NCT01187329), 97 patients underwent AVR for aortic stenosis. Of these patients, 95 had a standardized intraoperative transesophageal echocardiographic examination of systolic and diastolic function performed before surgical incision and repeated after chest closure. Echocardiographic images were analyzed off-line for global longitudinal myocardial strain and strain rate using 2D speckle-tracking echocardiography. Myocardial deformation assessed at the beginning of surgery was compared with the end of surgery using paired t tests corrected for multiple comparisons.
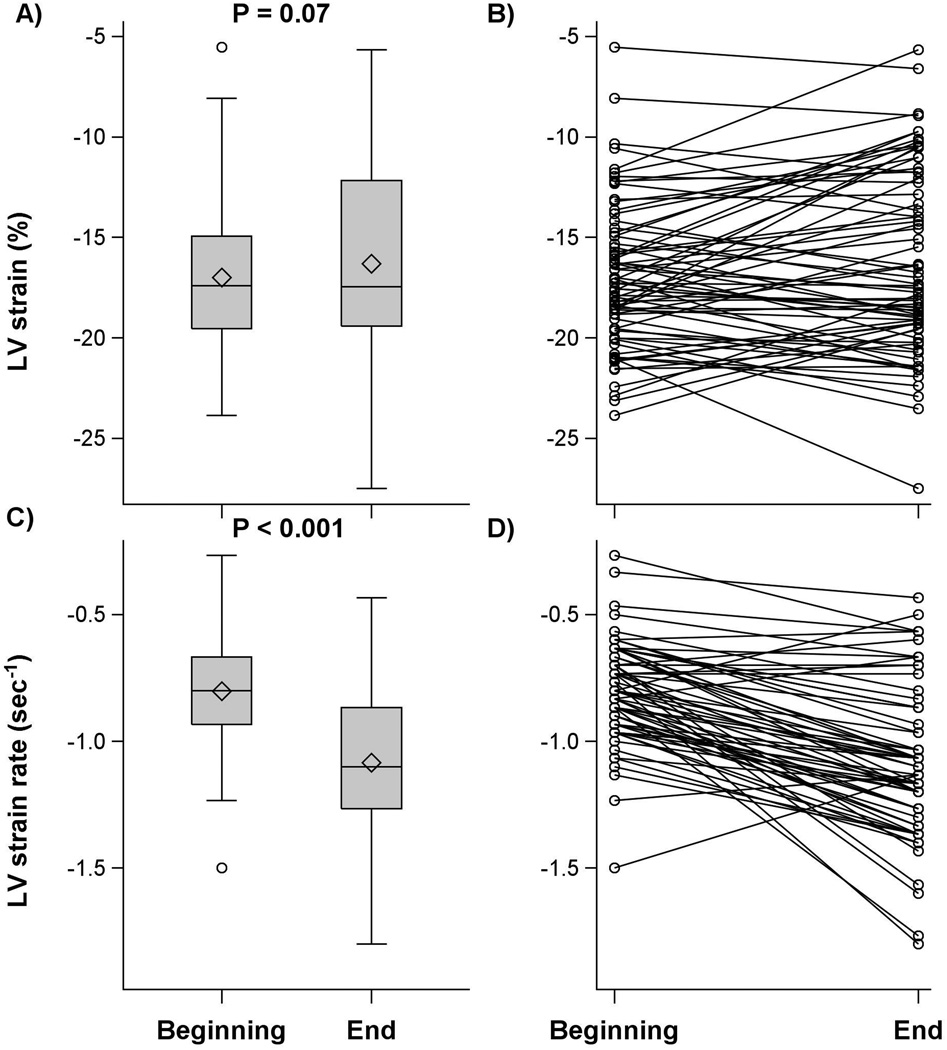
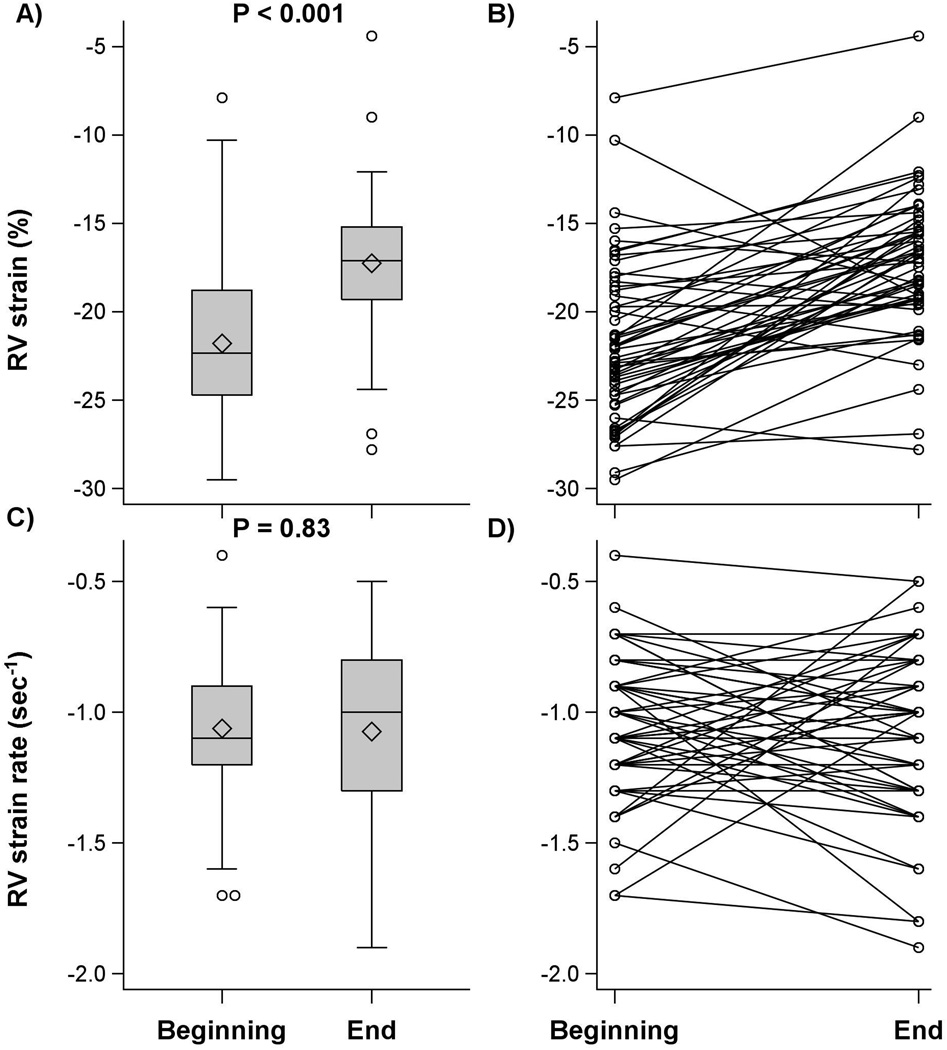
Results: LV volumes and arterial blood pressure decreased, and heart rate increased at the end of surgery. Echocardiographic images were acceptable for analysis in 72 patients for LV strain, 67 for LV strain rate, and 54 for RV strain and strain rate. In 72 patients with LV strain images, 9 patients required epinephrine, 22 required norepinephrine, and 2 required both at the end of surgery. LV strain did not change at the end of surgery compared with the beginning of surgery (difference: 0.7 [97.6% confidence interval, -0.2 to 1.5]%; P = 0.07), whereas LV systolic strain rate improved (became more negative) (-0.3 [-0.4 to -0.2] s; P < 0.001). In contrast, RV systolic strain worsened (became less negative) at the end of surgery (difference: 4.6 [3.1 to 6.0]%; P < 0.001) although RV systolic strain rate was unchanged (0.0 [97.6% confidence interval, -0.1 to 0.1]; P = 0.83).
Conclusions: LV function improved after replacement of a stenotic aortic valve demonstrated by improved longitudinal strain rate. In contrast, RV function, assessed by longitudinal strain, was reduced.
Conflict of interest statement
Name: Andra E. Duncan, MD, MS Contribution: Andra Duncan was responsible for the study design, conduct of the study, data collection, data analysis, data interpretation, and manuscript preparation. Andra Duncan is the archival author. Attestation: Andra Duncan attests to the integrity of the original data and analysis and approved the final manuscript. Conflicts of Interest: None. Name: Sheryar Sarwar, MD Contribution: Sheryar Sarwar was responsible for data collection and manuscript preparation. Attestation: Sheryar Sarwar approved the final manuscript. Conflicts of Interest: None. Name: Babak Kateby Kashy, MD Contribution: Babak Kateby Kashy was responsible for data collection and manuscript preparation. Attestation: Babak Kateby Kashy approved the final manuscript. Conflicts of Interest: None. Name: Abraham Sonny, MD Contribution: Abraham Sonny was responsible for data collection and manuscript preparation. Attestation: Abraham Sonny approved the final manuscript. Conflicts of Interest: None. Name: Shiva Sale, MD Contribution: Shiva Sale was responsible for data collection and manuscript preparation. Attestation: Shiva Sale approved the final manuscript. Conflicts of Interest: None. Name: Andrej Alfirevic, MD Contribution: Andrej Alfirevic was responsible for data collection and manuscript preparation. Attestation: Andrej Alfirevic approved the final manuscript. Conflicts of Interest: None. Name: Dongsheng Yang, MS Contribution: Dongsheng Yang was responsible for data analysis and interpretation. Attestation: Dongsheng Yang approved the final manuscript. Conflicts of Interest: None. Name: James D. Thomas, MD Contribution: James Thomas was responsible for study design, conduct of study, data interpretation, and manuscript preparation. Attestation: James Thomas approved the final manuscript. Conflicts of Interest: None. Name: Marc Gillinov, MD Contribution: Marc Gillinov was responsible for conduct of study, data interpretation, and manuscript preparation. Attestation: Marc Gillinov approved the final manuscript. Conflicts of Interest: Marc Gillinov serves as a consultant for Edwards Lifesciences, Medtronic, Tendyne, Abbott, On-X, and PleuraFlow. Dr. Gillinov has served as a speaker and/or received honoraria from Edward Lifesciences, Medtronic, and Intuitive Surgical and receives research support from St. Jude Medical. Name: Daniel I. Sessler, MD Contribution: Daniel Sessler was responsible for study design, conduct of study, data interpretation, and manuscript preparation. Attestation: Daniel Sessler attests to the integrity of the original data and analysis and approved the final manuscript. Conflicts of Interest: None. This manuscript was handled by: Martin J. London, MD
Figures
Comment in
-
We Should Train for Strain.Anesth Analg. 2017 Feb;124(2):386-387. doi: 10.1213/ANE.0000000000001696. Anesth Analg. 2017. PMID: 28098686 No abstract available.
References
-
- Carabello BA. Introduction to Aortic Stenosis. Circulation Research. 2013;113:179–185. - PubMed
-
- Brennan JM, Edwards FH, Zhao Y, O'Brien SM, Douglas PS, Peterson ED Developing Evidence to Inform Decisions About Effectiveness-Aortic Valve Replacement Research T. Long-term survival after aortic valve replacement among high-risk elderly patients in the United States: insights from the Society of Thoracic Surgeons Adult Cardiac Surgery Database, 1991 to 2007. Circulation. 2012;126:1621–1629. - PubMed
-
- Vanky FB, Hakanson E, Svedjeholm R. Long-term consequences of postoperative heart failure after surgery for aortic stenosis compared with coronary surgery. Ann Thorac Surg. 2007;83:2036–2043. - PubMed
-
- Haddad F, Denault AY, Couture P, Cartier R, Pellerin M, Levesque S, Lambert J, Tardif J-C. Right Ventricular Myocardial Performance Index Predicts Perioperative Mortality or Circulatory Failure in High-Risk Valvular Surgery. Journal of the American Society of Echocardiography. 2007;20:1065–1072. x00E, ois. - PubMed
-
- Kouchoukos NT, Blackstone EH, Hanley FL, Kirklin JK. Cardiac Surgery. Fourth. Philadelphia: Elsevier Saunders; 2013. pp. 133–162.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
