

Polymicrobial intensive care unit-acquired pneumonia: prevalence, microbiology and outcome
- PMID: 26703094
- PMCID: PMC4699341
- DOI: 10.1186/s13054-015-1165-5
Polymicrobial intensive care unit-acquired pneumonia: prevalence, microbiology and outcome
Abstract
Background: Microbial aetiology of intensive care unit (ICU)-acquired pneumonia (ICUAP) determines antibiotic treatment and outcomes. The impact of polymicrobial ICUAP is not extensively known. We therefore investigated the characteristics and outcomes of polymicrobial aetiology of ICUAP.
Method: Patients with ICUAP confirmed microbiologically were prospectively compared according to identification of 1 (monomicrobial) or more (polymicrobial) potentially-pathogenic microorganisms. Microbes usually considered as non-pathogenic were not considered for the etiologic diagnosis. We assessed clinical characteristics, microbiology, inflammatory biomarkers and outcome variables.
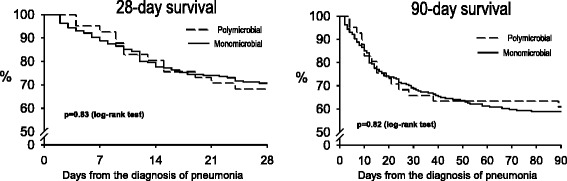
Results: Among 441 consecutive patients with ICUAP, 256 (58%) had microbiologic confirmation, and 41 (16%) of them polymicrobial pneumonia. Methicillin-sensitive Staphylococcus aureus, Haemophilus influenzae, and several Enterobacteriaceae were more frequent in polymicrobial pneumonia. Multi-drug and extensive-drug resistance was similarly frequent in both groups. Compared with monomicrobial, patients with polymicrobial pneumonia had less frequently chronic heart disease (6, 15% vs. 71, 33%, p = 0.019), and more frequently pleural effusion (18, 50%, vs. 54, 25%, p = 0.008), without any other significant difference. Appropriate empiric antimicrobial treatment was similarly frequent in the monomicrobial (185, 86%) and the polymicrobial group (39, 95%), as were the initial response to the empiric treatment, length of stay and mortality. Systemic inflammatory response was similar comparing monomicrobial with polymicrobial ICUAP.
Conclusion: The aetiology of ICUAP confirmed microbiologically was polymicrobial in 16% cases. Pleural effusion and absence of chronic heart disease are associated with polymicrobial pneumonia. When empiric treatment is frequently appropriate, polymicrobial aetiology does not influence the outcome of ICUAP.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
