

Predictors of lung function decline in scleroderma-related interstitial lung disease based on high-resolution computed tomography: implications for cohort enrichment in systemic sclerosis-associated interstitial lung disease trials
- PMID: 26704522
- PMCID: PMC4718035
- DOI: 10.1186/s13075-015-0872-2
Predictors of lung function decline in scleroderma-related interstitial lung disease based on high-resolution computed tomography: implications for cohort enrichment in systemic sclerosis-associated interstitial lung disease trials
Abstract
Background: The extent of lung involvement visualized by high-resolution computed tomography (HRCT) is a predictor of decline in forced vital capacity (FVC) in scleroderma-interstitial lung disease. Our objective was to evaluate the performance of three different HRCT-defined staging systems in the Scleroderma Lung Study I (SLS I) over a 1-year period.
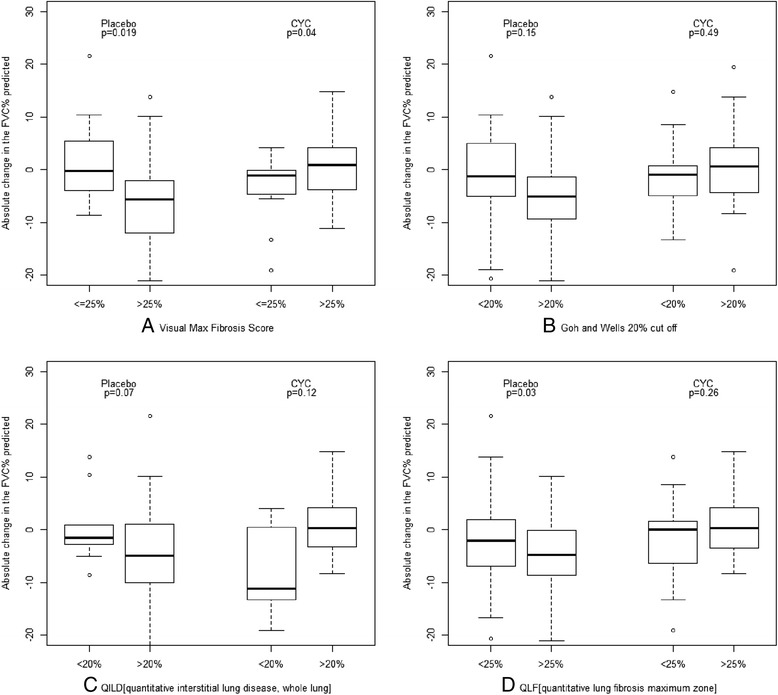
Methods: We assessed two visual semiquantitative scores: the maximum fibrosis score (MaxFib, the fibrosis score in the zone of maximal lung involvement) and visual assessment of total lung involvement (TLI) as proposed by Goh and Wells. In addition, we evaluated the computer-aided diagnosis and calculated the quantitative percentage with fibrosis (QLF) and TLI.
Results: The mean duration of the disease was 3.2 years, and the mean FVC was 67.7 %. Regardless of the staging system used, a greater degree of fibrosis/TLI on HRCT scans was associated with a greater decline in FVC in the placebo group. Using the MaxFib and QLF, the mean absolute changes in FVC from baseline were 0.1% and -1.4%, respectively, in <25% lung involvement vs. a change of -6.2% and -6.9%, respectively, with >25% involvement (negative score denotes worsening in FVC). Conversely, cyclophosphamide was able to stabilize decline in FVC in subjects with greater degree of involvement detected by HRCT. Using the visual MaxFib and QLF, the mean absolute improvements in FVC were 1.2 and 1.1, respectively, with >25% involvement.
Conclusions: HRCT-defined lung involvement was a predictor of decline in FVC in SLS I. The choice of staging system for cohort enrichment in a clinical trial depends on feasibility.
Trial registration: ClinicalTrials.gov identifier: NCT00004563 (Scleroderma Lung Study I) ISRCTN15982171. Registered 19 Aug 2015.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
