

Preoperative Safety Briefing Project
- PMID: 26704913
- PMCID: PMC4690713
- DOI: 10.7812/TPP/04.968
Preoperative Safety Briefing Project
Abstract
Context: Increased media attention on surgical procedures that were performed on the wrong anatomic site or wrong patient has prompted the health care industry to identify and address human factors that lead to medical errors.
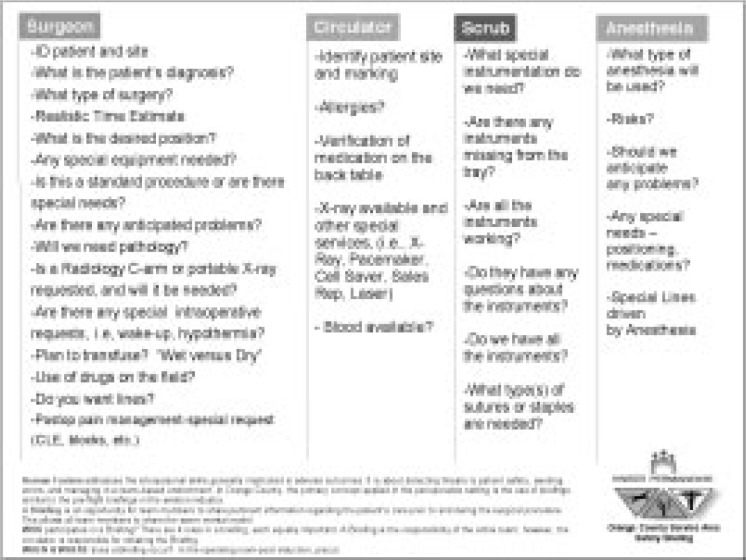
Objective: To increase patient safety in the perioperative setting, our objective was to create a climate of improved communication, collaboration, team-work, and situational awareness while the surgical team reviewed pertinent information about the patient and the pending procedure.
Methods: A team of doctors, nurses, and technicians used human factors principles to develop the Preoperative Safety Briefing for use by surgical teams, a briefing similar to the preflight checklist used by the airline industry. A six-month pilot of the briefing began in the Kaiser Permanente (KP) Anaheim Medical Center in February 2002. Four indicators of safety culture were used to measure success of the pilot: occurrence of wrong-site/wrong procedures, attitudinal survey data, near-miss reports, and nursing personnel turnover data.
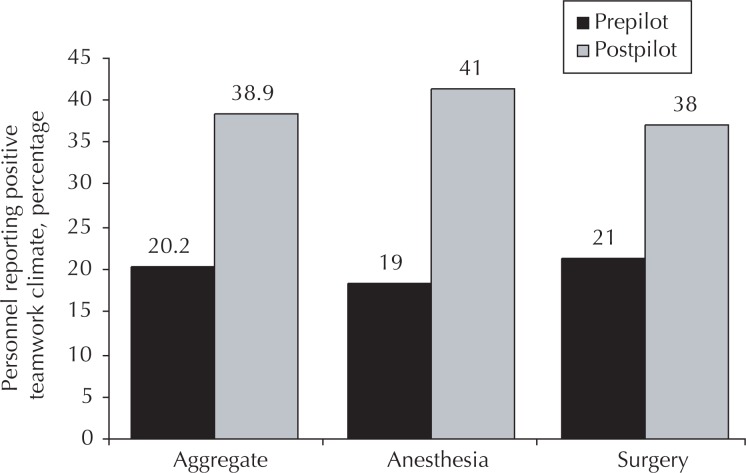
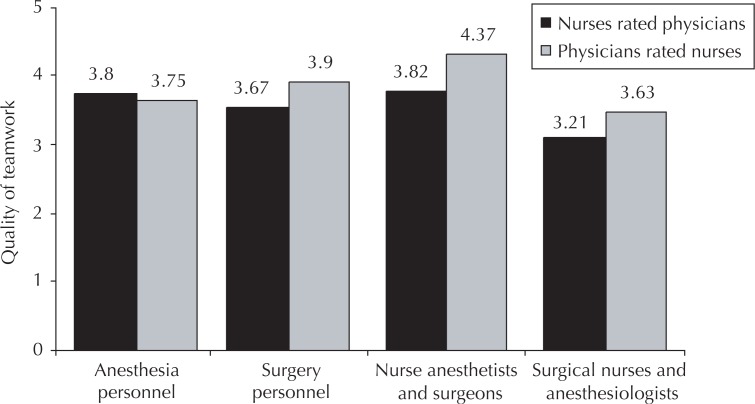
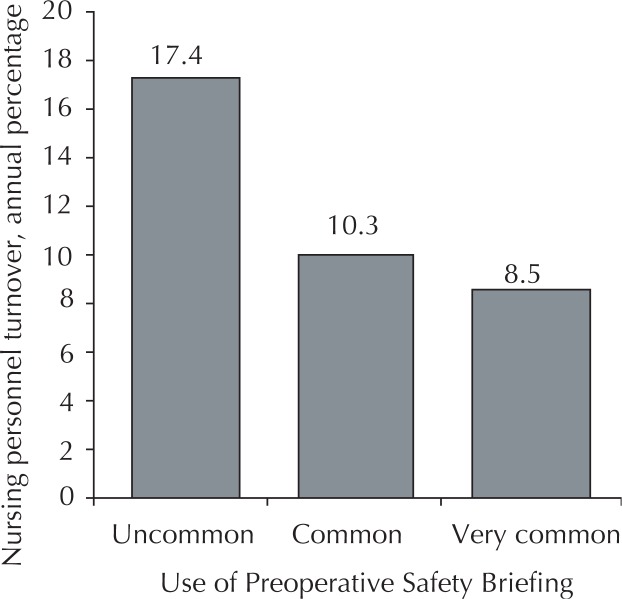
Results: Wrong-site surgeries decreased from 3 to 0 (300%) per year; employee satisfaction increased 19%; nursing personnel turnover decreased 16%; and perception of the safety climate in the operating room improved from "good" to "outstanding." Operating suite personnel perception of teamwork quality improved substantially. Operating suite personnel perception of patient safety as a priority, of personnel communication, of their taking responsibility for patient safety, of nurse input being well received, of overall morale, and of medical errors being handled appropriately also improved substantially.
Conclusions: Team members who work together and communicate well can quickly detect and more easily avoid errors. The Preoperative Safety Briefing is now standard in many operating suites in the KP Orange County Service Area. The concepts and design of this project are transferable, and similar projects are underway in the Departments of Radiology and of Labor and Delivery at KP Anaheim Medical Center.
Figures
References
-
- Institute of Medicine, Committee on Quality of Health Care in AmericaKohn LT, Corrigan JM, Donaldson MS, editors. To err is human: building a safer health system. Washington (DC): National Academic Press; 2000. Available from: www.nap.edu/openbook/0309068371/html/ (accessed March 18, 2004) - PubMed
-
- Leape LL. Error in medicine. JAMA. 1994 Dec 21;272(23):1851–7. - PubMed
-
- Joint Commission on Accreditation of Healthcare Organizations. Accredited organizations Hospitals. Sentinel event statistics. Jan 29, 2004. Available from: www.jcaho.org/accredited+organizations/hospitals/sentinel+events/sentine... (accessed March 17, 2004)
-
- Shortell SM, Zimmerman JE, Rousseau DM, et al. The performance of intensive care units: does good management make a difference? Med Care. 1994 May;32(5):508–25. - PubMed
-
- Young GJ, Charns MP, Daley J, Forbes MG, Henderson W, Khuri SF. Best practices for managing surgical services: the role of coordination. Health Care Manage Rev. 1997 Fall;22(4):72–81. - PubMed
LinkOut - more resources
Full Text Sources
