

Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities
- PMID: 26705059
- PMCID: PMC4718740
- DOI: 10.1016/j.yjmcc.2015.12.011
Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities
Abstract
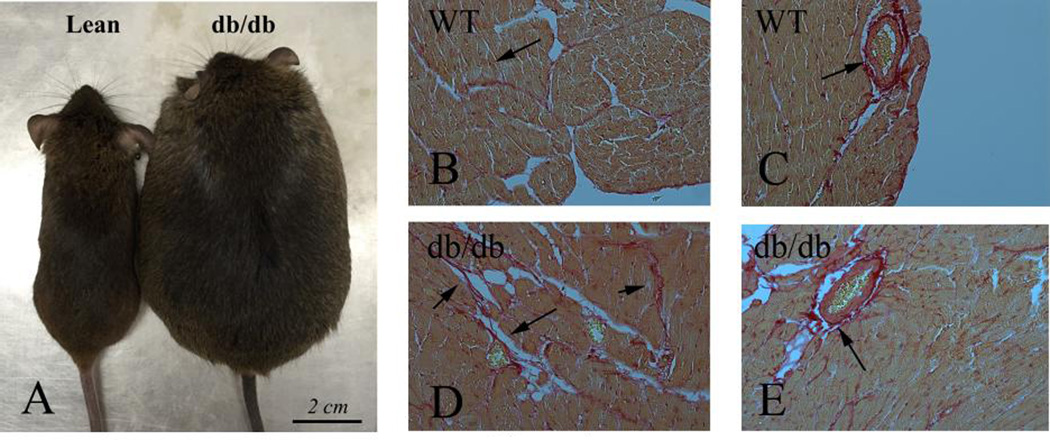
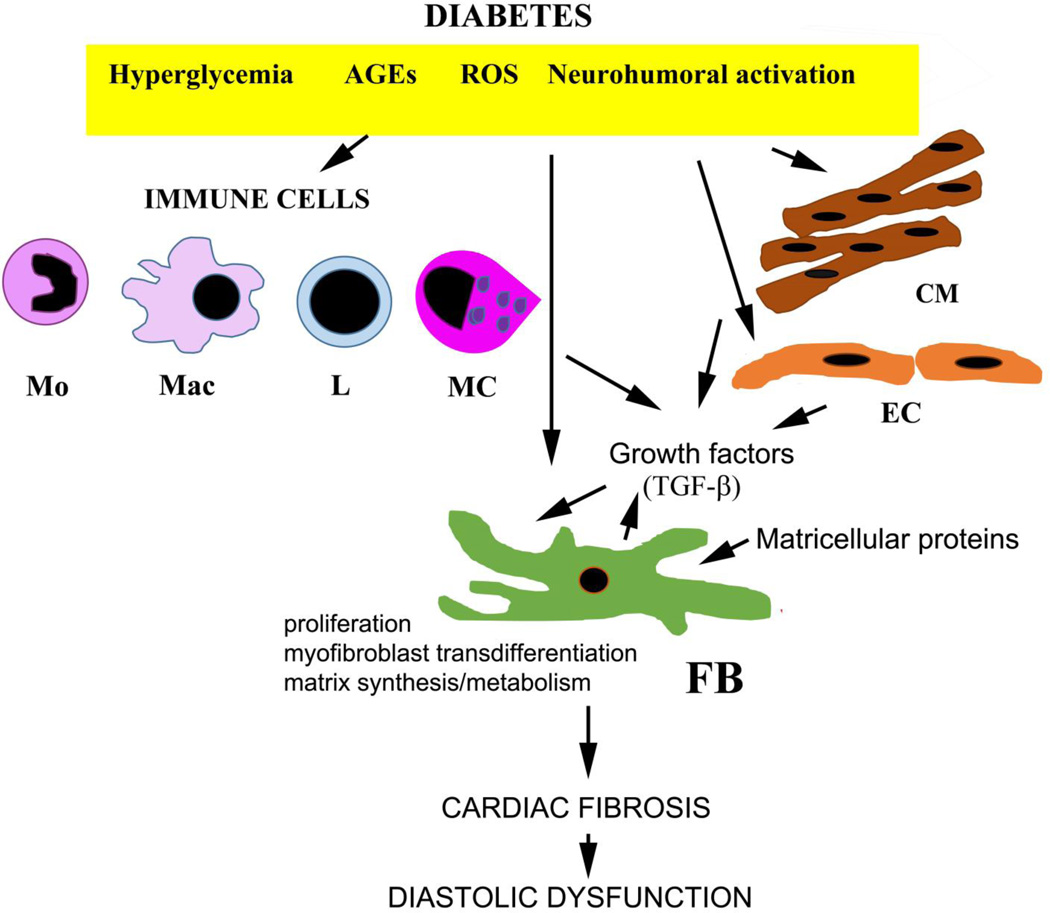
Both type 1 and type 2 diabetes are associated with cardiac fibrosis that may reduce myocardial compliance, contribute to the pathogenesis of heart failure, and trigger arrhythmic events. Diabetes-associated fibrosis is mediated by activated cardiac fibroblasts, but may also involve fibrogenic actions of macrophages, cardiomyocytes and vascular cells. The molecular basis responsible for cardiac fibrosis in diabetes remains poorly understood. Hyperglycemia directly activates a fibrogenic program, leading to accumulation of advanced glycation end-products (AGEs) that crosslink extracellular matrix proteins, and transduce fibrogenic signals through reactive oxygen species generation, or through activation of Receptor for AGEs (RAGE)-mediated pathways. Pro-inflammatory cytokines and chemokines may recruit fibrogenic leukocyte subsets in the cardiac interstitium. Activation of transforming growth factor-β/Smad signaling may activate fibroblasts inducing deposition of structural extracellular matrix proteins and matricellular macromolecules. Adipokines, endothelin-1 and the renin-angiotensin-aldosterone system have also been implicated in the diabetic myocardium. This manuscript reviews our current understanding of the cellular effectors and molecular pathways that mediate fibrosis in diabetes. Based on the pathophysiologic mechanism, we propose therapeutic interventions that may attenuate the diabetes-associated fibrotic response and discuss the challenges that may hamper clinical translation.
Keywords: Diabetes; Fibroblast; Fibrosis; Heart failure; Obesity.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Cardiac fibrosis: Cell biological mechanisms, molecular pathways and therapeutic opportunities.Mol Aspects Med. 2019 Feb;65:70-99. doi: 10.1016/j.mam.2018.07.001. Epub 2018 Aug 2. Mol Aspects Med. 2019. PMID: 30056242 Review.
-
Cardiac fibrosis.Cardiovasc Res. 2021 May 25;117(6):1450-1488. doi: 10.1093/cvr/cvaa324. Cardiovasc Res. 2021. PMID: 33135058 Free PMC article. Review.
-
Fibroblasts and the extracellular matrix in right ventricular disease.Cardiovasc Res. 2017 Oct 1;113(12):1453-1464. doi: 10.1093/cvr/cvx146. Cardiovasc Res. 2017. PMID: 28957531 Free PMC article. Review.
-
Fibrosis of the diabetic heart: Clinical significance, molecular mechanisms, and therapeutic opportunities.Adv Drug Deliv Rev. 2021 Sep;176:113904. doi: 10.1016/j.addr.2021.113904. Epub 2021 Jul 29. Adv Drug Deliv Rev. 2021. PMID: 34331987 Free PMC article. Review.
-
Advanced Glycation End Products Enhance Macrophages Polarization into M1 Phenotype through Activating RAGE/NF-κB Pathway.Biomed Res Int. 2015;2015:732450. doi: 10.1155/2015/732450. Epub 2015 May 31. Biomed Res Int. 2015. PMID: 26114112 Free PMC article.
Cited by
-
Activation of calcium‑sensing receptor‑mediated autophagy in high glucose‑induced cardiac fibrosis in vitro.Mol Med Rep. 2020 Sep;22(3):2021-2031. doi: 10.3892/mmr.2020.11277. Epub 2020 Jun 26. Mol Med Rep. 2020. PMID: 32705187 Free PMC article.
-
Research advances in the therapy of metabolic syndrome.Front Pharmacol. 2024 Jul 30;15:1364881. doi: 10.3389/fphar.2024.1364881. eCollection 2024. Front Pharmacol. 2024. PMID: 39139641 Free PMC article. Review.
-
Calcium‑sensing receptor promotes high glucose‑induced myocardial fibrosis via upregulation of the TGF‑β1/Smads pathway in cardiac fibroblasts.Mol Med Rep. 2019 Aug;20(2):1093-1102. doi: 10.3892/mmr.2019.10330. Epub 2019 Jun 4. Mol Med Rep. 2019. PMID: 31173208 Free PMC article.
-
Non-ischemic dilated cardiomyopathy and cardiac fibrosis.Heart Fail Rev. 2021 Sep;26(5):1081-1101. doi: 10.1007/s10741-020-09940-0. Heart Fail Rev. 2021. PMID: 32170530 Review.
-
Cardiac fibroblast activation and hyaluronan synthesis in response to hyperglycemia and diet-induced insulin resistance.Sci Rep. 2019 Feb 12;9(1):1827. doi: 10.1038/s41598-018-36140-6. Sci Rep. 2019. PMID: 30755628 Free PMC article.
References
-
- Gilbert RE, Krum H. Heart failure in diabetes: effects of anti-hyperglycaemic drug therapy. Lancet. 2015;385:2107–2117. - PubMed
-
- Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34:29–34. - PubMed
-
- Cavender MA, Steg PG, Smith SC, Jr, Eagle K, Ohman EM, Goto S, et al. Impact of Diabetes Mellitus on Hospitalization for Heart Failure, Cardiovascular Events, and Death: Outcomes at 4 Years From the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Circulation. 2015;132:923–931. - PubMed
-
- MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29:1377–1385. - PubMed
-
- Bell DS. Heart failure: the frequent, forgotten, and often fatal complication of diabetes. Diabetes Care. 2003;26:2433–2441. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
