

Optimizing treatment success in multiple sclerosis
- PMID: 26705122
- PMCID: PMC4893374
- DOI: 10.1007/s00415-015-7986-y
Optimizing treatment success in multiple sclerosis
Abstract
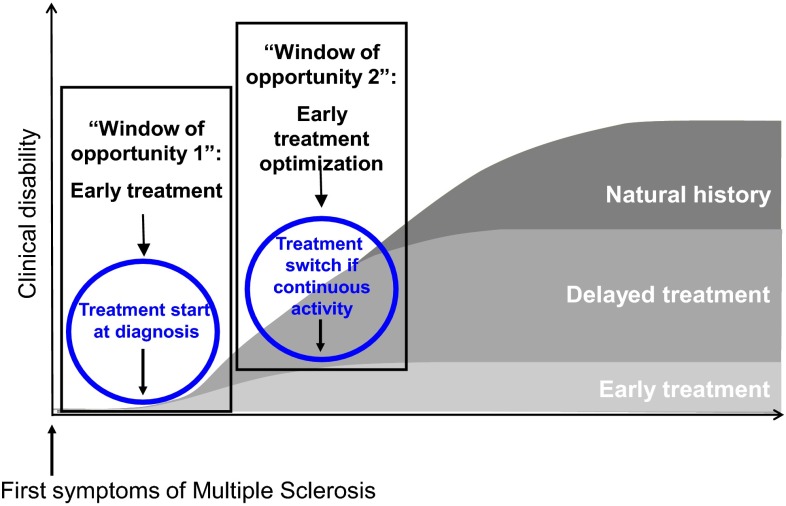
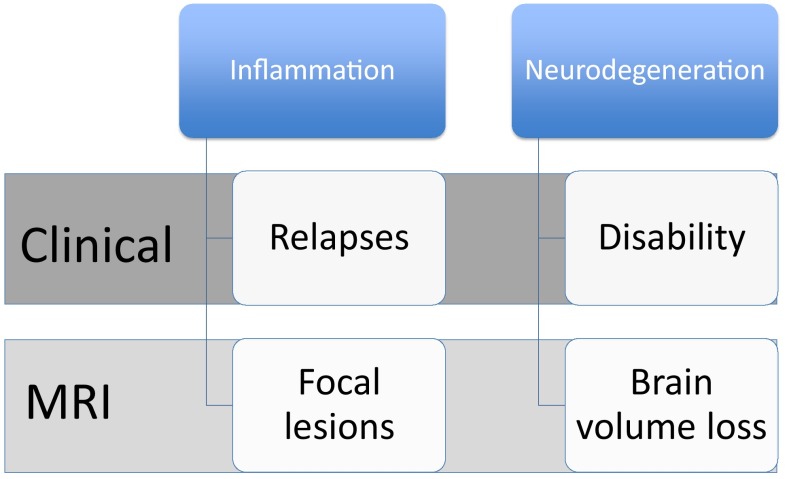
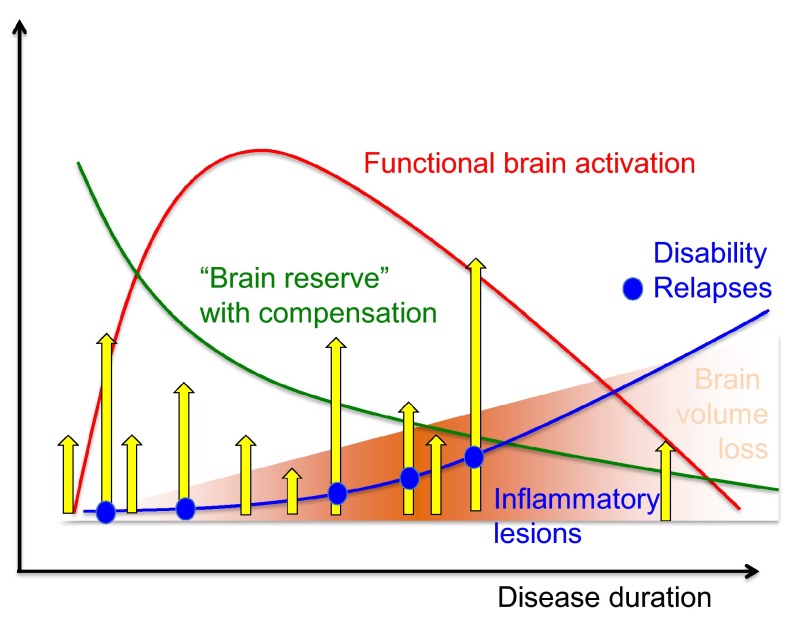
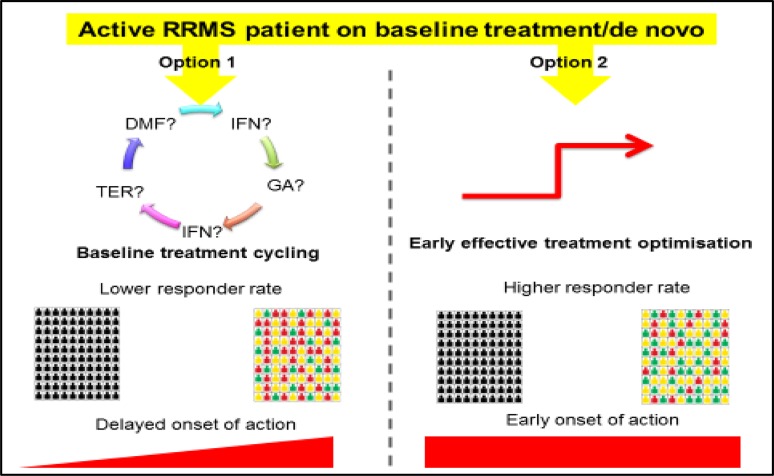
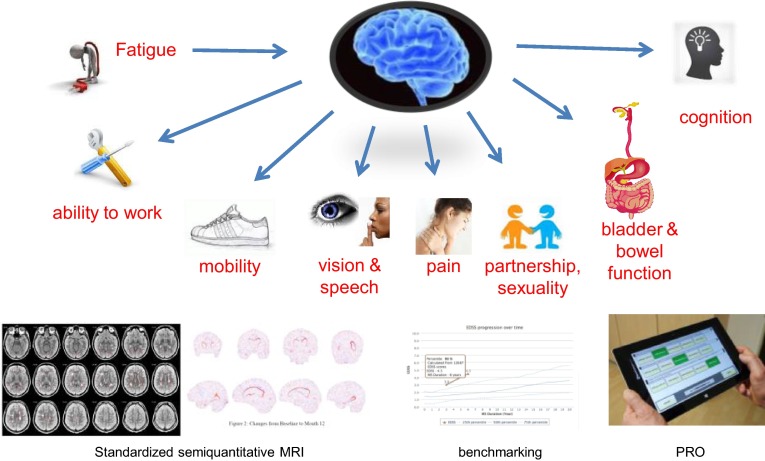
Despite important advances in the treatment of multiple sclerosis (MS) over recent years, the introduction of several disease-modifying therapies (DMTs), the burden of progressive disability and premature mortality associated with the condition remains substantial. This burden, together with the high healthcare and societal costs associated with MS, creates a compelling case for early treatment optimization with highly efficacious therapies. Often, patients receive several first-line therapies, while more recent and in part more effective treatments are still being introduced only after these have failed. However, with the availability of highly efficacious therapies, a novel treatment strategy has emerged, where the aim is to achieve no evidence of disease activity (NEDA). Achieving NEDA necessitates regular monitoring of relapses, disability and functionality. However, there is only a poor correlation between conventional magnetic resonance imaging measures like T2 hyperintense lesion burden and the level of clinical disability. Hence, MRI-based measures of brain atrophy have emerged in recent years potentially reflecting the magnitude of MS-related neuroaxonal damage. Currently available DMTs differ markedly in their effects on brain atrophy: some, such as fingolimod, have been shown to significantly slow brain volume loss, compared to placebo, whereas others have shown either no, inconsistent, or delayed effects. In addition to regular monitoring, treatment optimization also requires early intervention with efficacious therapies, because accumulating evidence shows that effective intervention during a limited period early in the course of MS is critical for maintaining neurological function and preventing subsequent disability. Together, the advent of new MS therapies and evolving management strategies offer exciting new opportunities to optimize treatment outcomes.
Keywords: Brain atrophy; Disability evaluation; Drug therapy; Multiple sclerosis.
Figures
References
-
- Ziemssen T. Multiple sclerosis beyond EDSS: depression and fatigue. J Neurol Sci. 2009;277(Suppl 1):S37–S41. - PubMed
-
- Rao SM, Leo GJ, Bernardin L, Unverzagt F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology. 2009;41:685–691. - PubMed
-
- Rao SM, Leo GJ, Ellington L, Nauertz T, Bernardin L, Unverzagt F. Cognitive dysfunction in multiple sclerosis. II. Impact on employment and social functioning. Neurology. 1991;41:692–696. - PubMed
-
- Potagas C, Giogkaraki E, Koutsis G, Mandellos D, Tsirempolou E, Sfagos C, Vassilopoulos D. Cognitive impairment in different MS subtypes and clinically isolated syndromes. J Neurol Sci. 2008;267:100–106. - PubMed
-
- Feuillet L, Reuter F, Audoin B, Malikova I, Barrau K, Cherif AA, Pelletier J. Early cognitive impairment in patients with clinically isolated syndrome suggestive of multiple sclerosis. Mult Scler. 2007;13:124–127. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
