

The value of basic research insights into atrial fibrillation mechanisms as a guide to therapeutic innovation: a critical analysis
- PMID: 26705366
- PMCID: PMC4777910
- DOI: 10.1093/cvr/cvv275
The value of basic research insights into atrial fibrillation mechanisms as a guide to therapeutic innovation: a critical analysis
Abstract
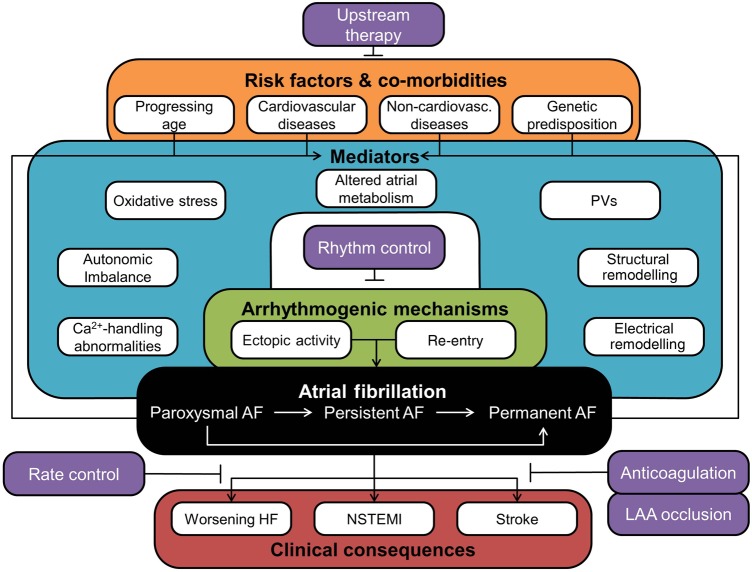
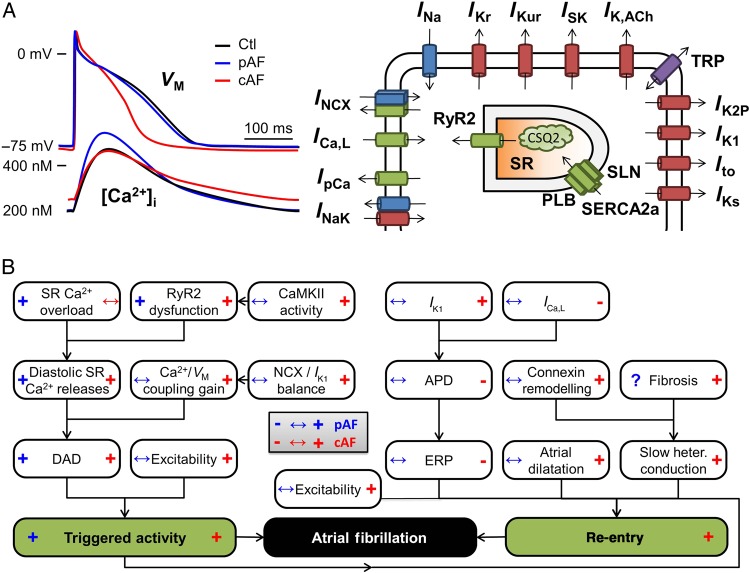
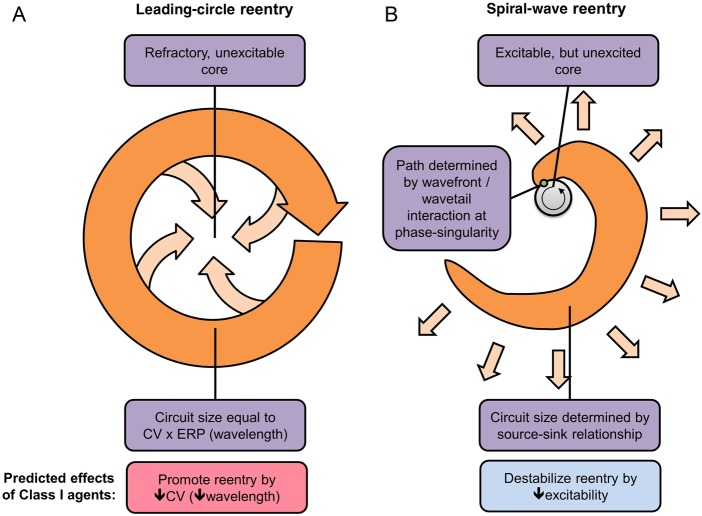
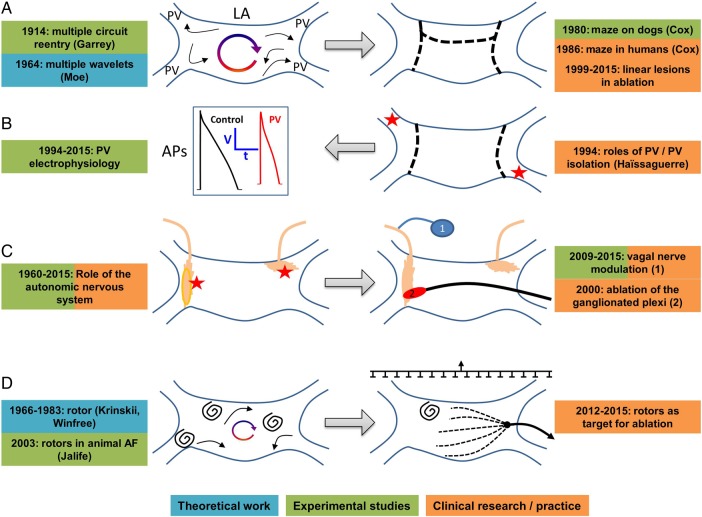
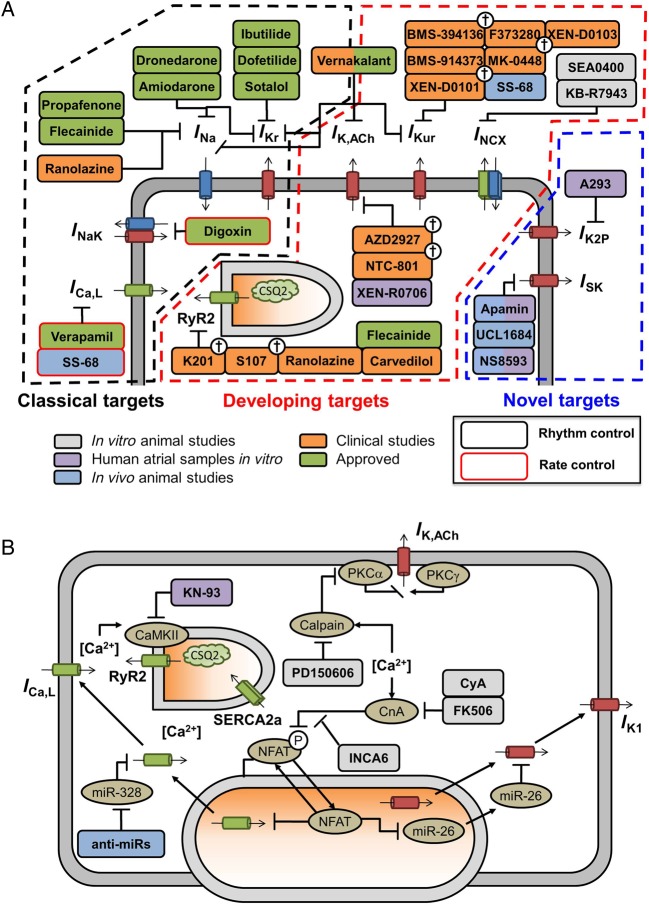
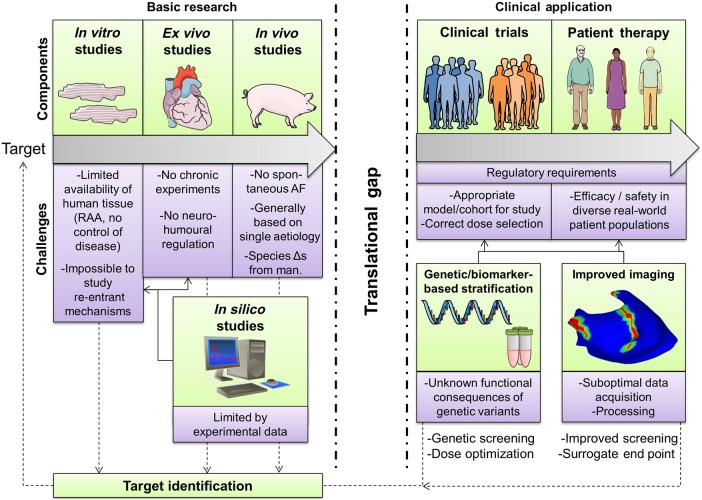
Atrial fibrillation (AF) is an extremely common clinical problem associated with increased morbidity and mortality. Current antiarrhythmic options include pharmacological, ablation, and surgical therapies, and have significantly improved clinical outcomes. However, their efficacy remains suboptimal, and their use is limited by a variety of potentially serious adverse effects. There is a clear need for improved therapeutic options. Several decades of research have substantially expanded our understanding of the basic mechanisms of AF. Ectopic firing and re-entrant activity have been identified as the predominant mechanisms for arrhythmia initiation and maintenance. However, it has become clear that the clinical factors predisposing to AF and the cellular and molecular mechanisms involved are extremely complex. Moreover, all AF-promoting and maintaining mechanisms are dynamically regulated and subject to remodelling caused by both AF and cardiovascular disease. Accordingly, the initial presentation and clinical progression of AF patients are enormously heterogeneous. An understanding of arrhythmia mechanisms is widely assumed to be the basis of therapeutic innovation, but while this assumption seems self-evident, we are not aware of any papers that have critically examined the practical contributions of basic research into AF mechanisms to arrhythmia management. Here, we review recent insights into the basic mechanisms of AF, critically analyse the role of basic research insights in the development of presently used anti-AF therapeutic options and assess the potential value of contemporary experimental discoveries for future therapeutic innovation. Finally, we highlight some of the important challenges to the translation of basic science findings to clinical application.
Keywords: Ablation; Antiarrhythmic drugs; Atrial fibrillation; Cellular electrophysiology; Ectopic activity; Imaging; Re-entry.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Nattel S. New ideas about atrial fibrillation 50 years on. Nature 2002;415:219–226. - PubMed
-
- Nishida K, Nattel S. Atrial fibrillation compendium: historical context and detailed translational perspective on an important clinical problem. Circ Res 2014;114:1447–1452. - PubMed
-
- Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res 2014;114:1453–1468. - PubMed
-
- Dobrev D, Nattel S. New antiarrhythmic drugs for treatment of atrial fibrillation. Lancet 2010;375:1212–1223. - PubMed
-
- Heijman J, Voigt N, Dobrev D. New directions in antiarrhythmic drug therapy for atrial fibrillation. Future Cardiol 2013;9:71–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
