

All-cause mortality by age and gender based on coronary artery calcium scores
- PMID: 26705490
- PMCID: PMC6392424
- DOI: 10.1093/ehjci/jev328
All-cause mortality by age and gender based on coronary artery calcium scores
Abstract
Aims: Although coronary artery calcium (CAC) has been established as a robust tool for predicting total mortality during intermediate follow-up, less is known about the long-term predictive value of CAC.
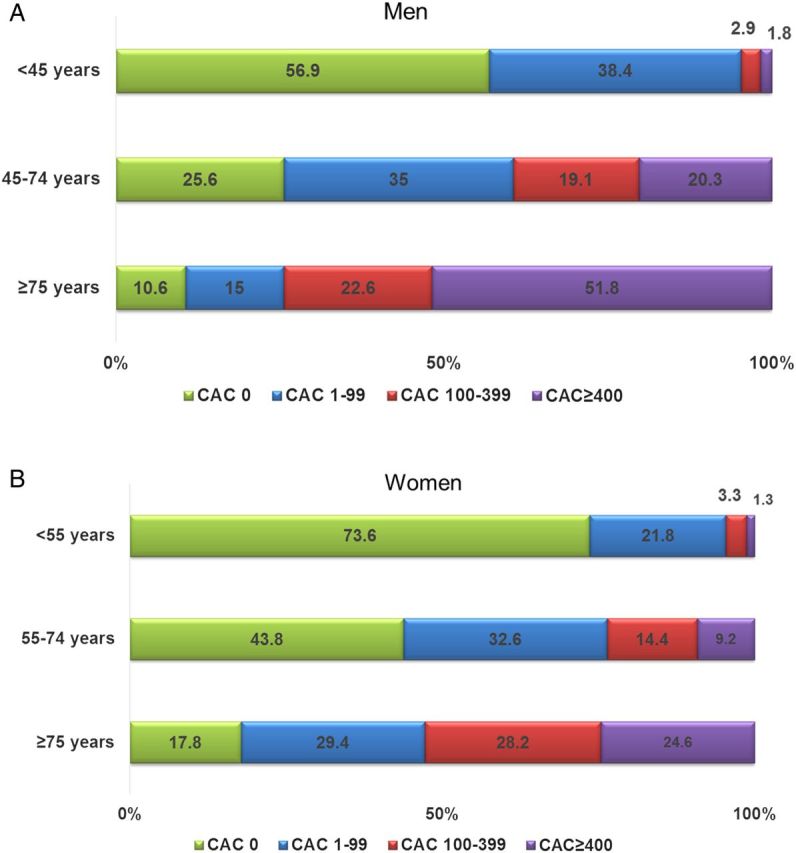
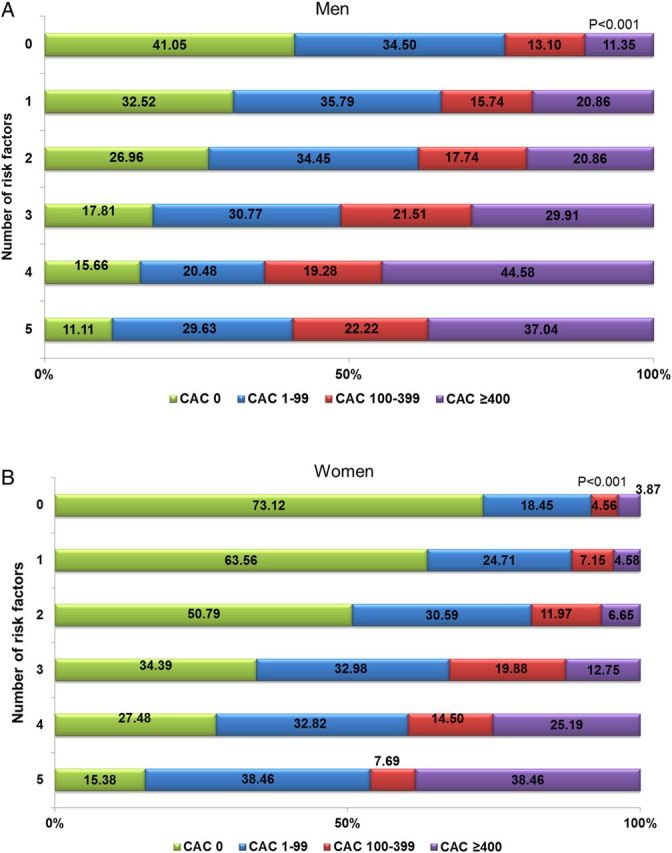
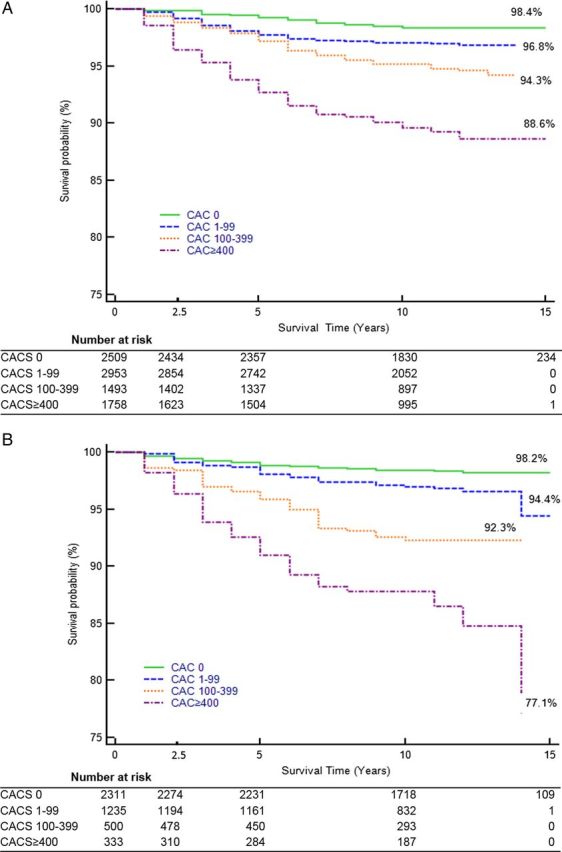
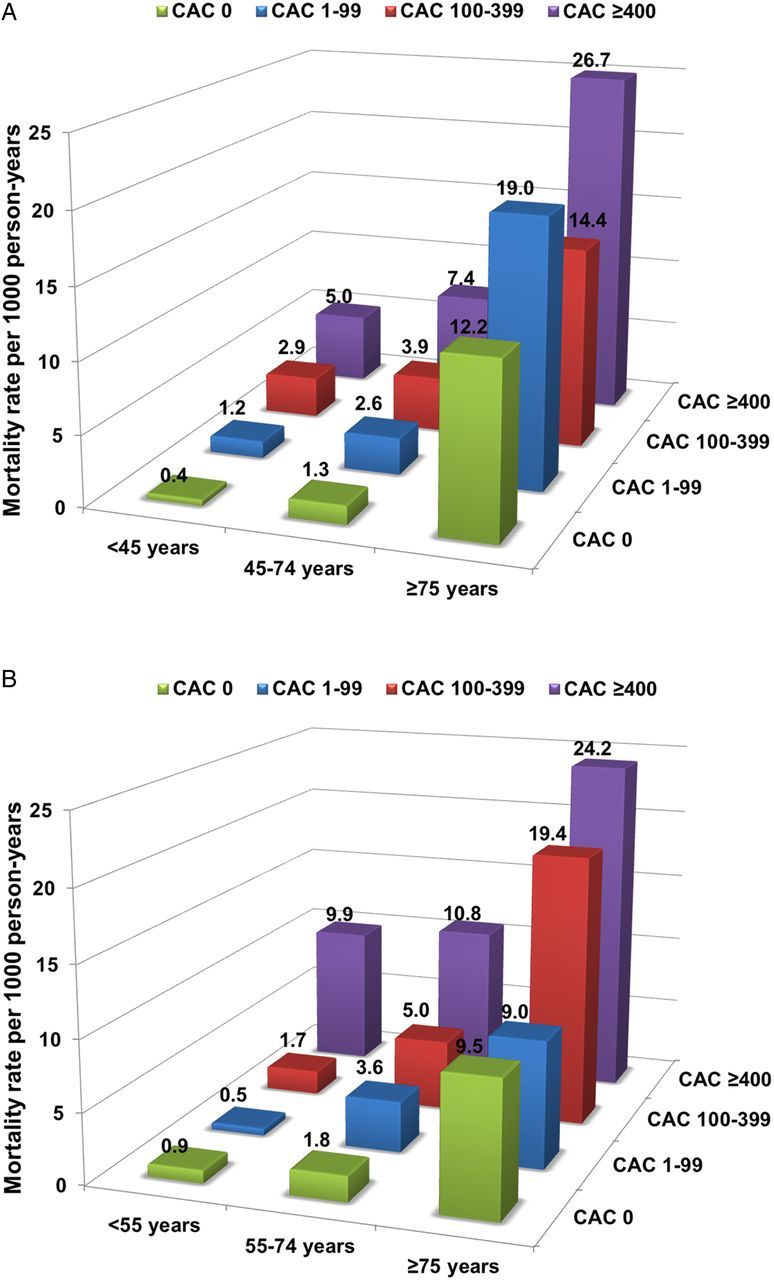
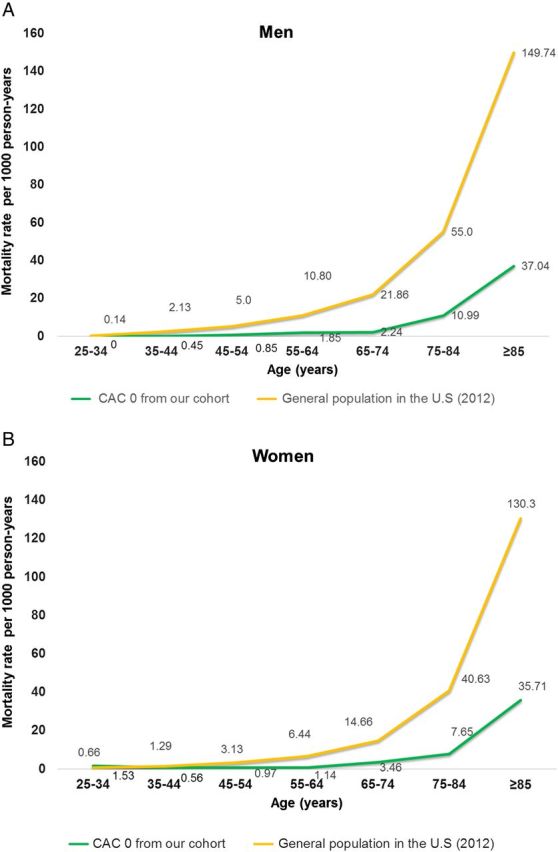
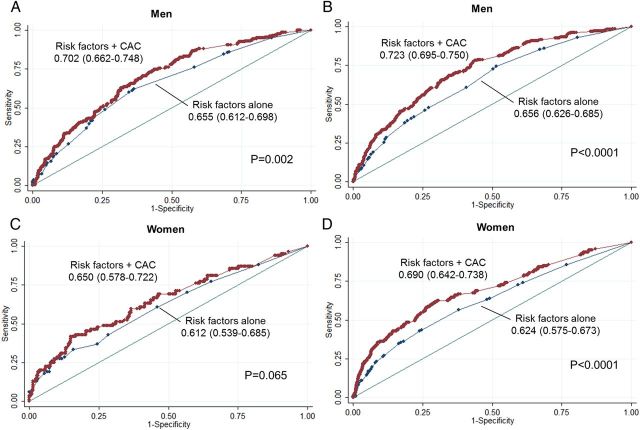
Methods and results: This study included 13 092 asymptomatic patients without known cardiovascular disease who underwent a clinically indicated CAC scan. CAC was categorized as an Agatson score of 0, 1-99, 100-399, and ≥400. We used multivariable Cox proportional hazards to calculate adjusted hazard ratios (HRs) for mortality stratified by age (younger, intermediate, or older) and gender. The mean age of participants was 58 ± 11 years and 67% were men. During a median follow-up of 11.0 ± 3.2 years, there were 522 deaths (4.0%). Compared with CAC = 0, increasing CAC was associated with higher mortality rate: 1-99 [HR: 1.5, 95% confidence interval (95% CI): 1.1-2.1]; 100-399 (HR: 1.8, 95% CI: 1.3-2.5); ≥400 (HR: 2.6, 95% CI: 1.9-3.6). Relative risk according to CAC category did not differ between genders. The strongest associations between CAC and mortality were observed for young and intermediate age participants. Nonetheless, the mortality rate of the older patients with CAC = 0 was far lower than that of the general US population. CAC was more predictive of long-term (15 years) than intermediate-term (5 years) mortality for men [receiver operator characteristics (ROC): 0.723 vs. 0.702] and women (ROC: 0.69 vs. 0.65).
Conclusion: CAC is strongly associated with the long-term risk of mortality in young- and middle-aged men and women. In older patients, the long-term risk stratification of CAC is lower, due principally to increased mortality rate in patients with low calcium scores; however, even in the older patients, those with absent or low CAC are at a significantly lower risk of mortality compared with the general population.
Keywords: Age; Coronary artery calcium score; Gender; Long-term mortality; Mortality risk.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ et al. Executive summary: heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation 2014;129:399–410. - PubMed
-
- Kavousi M, Leening MJ, Nanchen D, Greenland P, Graham IM, Steyerberg EW et al. Comparison of application of the ACC/AHA guidelines, adult treatment panel III guidelines, and European Society of Cardiology guidelines for cardiovascular disease prevention in a European cohort. JAMA 2014;311:1416–23. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American college of cardiology/American heart association task force on practice guidelines. J Am Coll Cardiol 2014;63:2889–934. - PubMed
-
- Budoff MJ, Shaw LJ, Liu ST, Weinstein SR, Mosler TP, Tseng PH et al. Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol 2007;49:1860–70. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
