

Circulation detection using the electrocardiogram and the thoracic impedance acquired by defibrillation pads
- PMID: 26705970
- PMCID: PMC4724594
- DOI: 10.1016/j.resuscitation.2015.11.014
Circulation detection using the electrocardiogram and the thoracic impedance acquired by defibrillation pads
Abstract
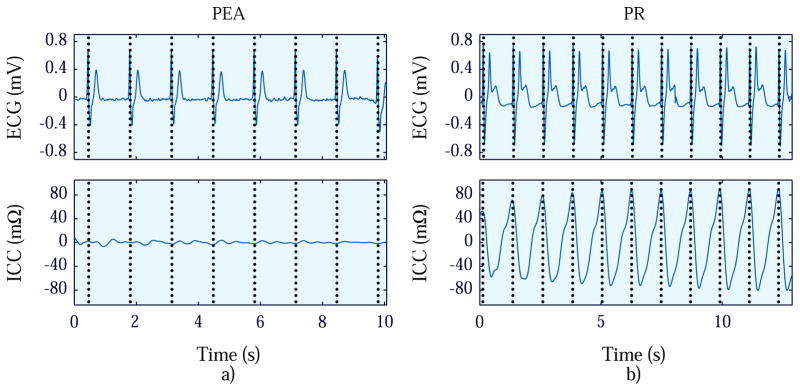
Aim: To develop and evaluate a method to detect circulation in the presence of organized rhythms (ORs) during resuscitation using signals acquired by defibrillation pads.
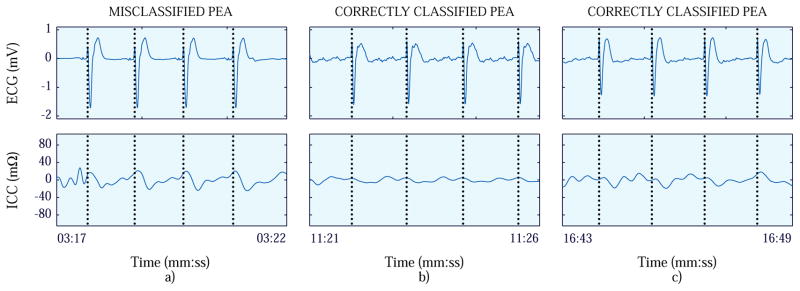
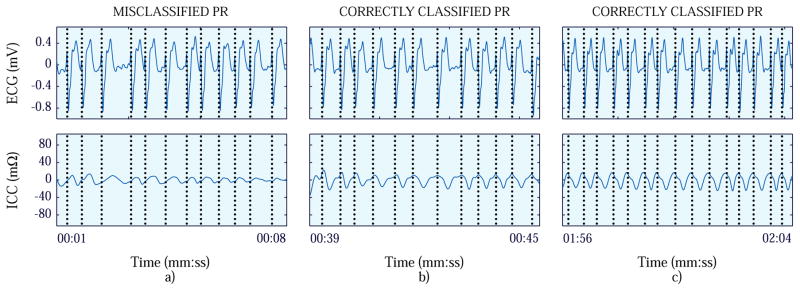
Methods: Segments containing electrocardiogram (ECG) and thoracic impedance (TI) signals free of artifacts were used. The ECG corresponded to ORs classified as pulseless electrical activity (PEA) or pulse-generating rhythm (PR). A first dataset containing 1091 segments was split into training and test sets to develop and validate the circulation detector. The method processed ECG and TI to obtain the impedance circulation component (ICC). Morphological features were extracted from ECG and ICC, and combined into a classifier to discriminate between PEA and PR. The performance of the method was evaluated in terms of sensitivity (PR) and specificity (PEA). A second dataset (86 segments from different patients) was used to assess two application of the method: confirmation of arrest by recognizing absence of circulation during ORs and detection of return of spontaneous circulation (ROSC) during resuscitation. In both cases, time to confirmation of arrest/ROSC was determined.
Results: The method showed a sensitivity/specificity of 92.1%/90.3% and 92.2%/91.9% for training and test sets respectively. The method confirmed cardiac arrest with a specificity of 93.3% with a median delay of 0s after the first OR annotation. ROSC was detected with a sensitivity of 94.4% with a median delay of 57s from ROSC onset.
Conclusion: The method showed good performance, and can be reliably used to distinguish perfusing from non-perfusing ORs.
Keywords: Circulation detection; Defibrillator; Pulse; Pulse-generating rhythm; Pulseless electrical activity; Thoracic impedance.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Mohamud Daya is an unpaid consultant for Philips Healthcare.
Figures


Similar articles
-
Reliable extraction of the circulation component in the thoracic impedance measured by defibrillation pads.Resuscitation. 2013 Oct;84(10):1345-52. doi: 10.1016/j.resuscitation.2013.05.020. Epub 2013 Jun 4. Resuscitation. 2013. PMID: 23747932
-
Circulation assessment by automated external defibrillators during cardiopulmonary resuscitation.Resuscitation. 2018 Jul;128:158-163. doi: 10.1016/j.resuscitation.2018.04.036. Epub 2018 May 4. Resuscitation. 2018. PMID: 29733921
-
Capnography: A support tool for the detection of return of spontaneous circulation in out-of-hospital cardiac arrest.Resuscitation. 2019 Sep;142:153-161. doi: 10.1016/j.resuscitation.2019.03.048. Epub 2019 Apr 18. Resuscitation. 2019. PMID: 31005583
-
Pulseless electrical activity in cardiac arrest: electrocardiographic presentations and management considerations based on the electrocardiogram.Am J Emerg Med. 2012 Jan;30(1):236-9. doi: 10.1016/j.ajem.2010.08.017. Epub 2010 Oct 20. Am J Emerg Med. 2012. PMID: 20970286 Review.
-
Pseudo-pulseless electrical activity in the emergency department, an evidence based approach.Am J Emerg Med. 2020 Feb;38(2):371-375. doi: 10.1016/j.ajem.2019.158503. Epub 2019 Oct 14. Am J Emerg Med. 2020. PMID: 31740090 Review.
Cited by
-
Transthoracic Impedance Measured with Defibrillator Pads-New Interpretations of Signal Change Induced by Ventilations.J Clin Med. 2019 May 22;8(5):724. doi: 10.3390/jcm8050724. J Clin Med. 2019. PMID: 31121817 Free PMC article.
-
Detection of spontaneous pulse using the acceleration signals acquired from CPR feedback sensor in a porcine model of cardiac arrest.PLoS One. 2017 Dec 8;12(12):e0189217. doi: 10.1371/journal.pone.0189217. eCollection 2017. PLoS One. 2017. PMID: 29220414 Free PMC article.
-
Assessment of the evolution of end-tidal carbon dioxide within chest compression pauses to detect restoration of spontaneous circulation.PLoS One. 2021 May 18;16(5):e0251511. doi: 10.1371/journal.pone.0251511. eCollection 2021. PLoS One. 2021. PMID: 34003839 Free PMC article. Clinical Trial.
-
Pulseless Electric Activity or Electromechanical Dissociation.Circ Arrhythm Electrophysiol. 2024 Feb;17(2):e012760. doi: 10.1161/CIRCEP.124.012760. Epub 2024 Feb 6. Circ Arrhythm Electrophysiol. 2024. PMID: 38318697 Free PMC article. No abstract available.
-
Cardiac output estimation using ballistocardiography: a feasibility study in healthy subjects.Sci Rep. 2024 Jan 19;14(1):1671. doi: 10.1038/s41598-024-52300-3. Sci Rep. 2024. PMID: 38238507 Free PMC article.
References
-
- Perkins GD, Stephenson B, Hulme J, Monsieurs KG. Birmingham assessment of breathing study (BABS) Resuscitation. 2005;64(1):109–113. - PubMed
-
- Ruppert M, Reith MW, Widmann JH, et al. Checking for breathing: evaluation of the diagnostic capability of emergency medical services personnel, physicians, medical students, and medical laypersons. Annals of Emergency Medicine. 1999;34(6):720–729. - PubMed
-
- Bossaert L, Handley A, Marsden A, et al. European Resuscitation Council guidelines for the use of automated external defibrillators by EMS providers and first responders: A statement from the Early Defibrillation Task Force, with contributions from the Working Groups on Basic and Advanced Life Support, and approved by the Executive Committee of the European Resuscitation. Resuscitation. 1998;37(2):91–94. - PubMed
-
- Eberle B, Dick WF, Schneider T, Wisser G, Doetsch S, Tzanova I. Checking the carotid pulse check: diagnostic accuracy of first responders in patients with and without a pulse. Resuscitation. 1996;33(2):107–116. - PubMed
-
- Ochoa FJ, Ramalle-Gómara E, Carpintero JM, García A, Saralegui I. Competence of health professionals to check the carotid pulse. Resuscitation. 1998;37(3):173–175. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
