

Dynamic Contrast-Enhanced MRI in Low-Grade Versus Anaplastic Oligodendrogliomas
- PMID: 26707628
- PMCID: PMC5510484
- DOI: 10.1111/jon.12320
Dynamic Contrast-Enhanced MRI in Low-Grade Versus Anaplastic Oligodendrogliomas
Abstract
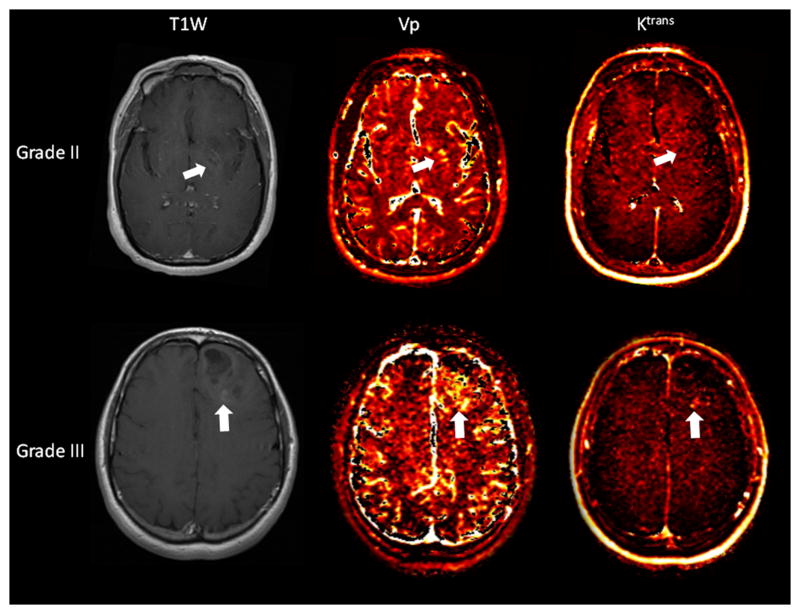
Background and purpose: Low-grade and anaplastic oligodendrogliomas are often difficult to differentiate on the basis of conventional MR imaging characteristics. Dynamic contrast-enhanced (DCE) MRI can assess tumor microvasculature and has demonstrated utility for predicting glioma grade and prognosis in primary brain tumors. The aim of our study was to evaluate the performance of plasma volume (Vp) and volume transfer coefficient (K(trans) ) derived from DCE MRI in differentiating between grade II and grade III oligodendrogliomas.
Materials and methods: Twenty-four consecutive patients with pathologically confirmed oligodendroglioma (World Health Organization grade II, n = 14 and grade III, n = 10) were retrospectively assessed. Pretreatment DCE MRI was performed and regions of interest were manually drawn around the entire tumor volume to calculate Vp and K(trans) . The Mann-Whitney U test and receiver operating characteristic (ROC) analysis were performed to compare pharmacokinetic parameters between the 2 groups.
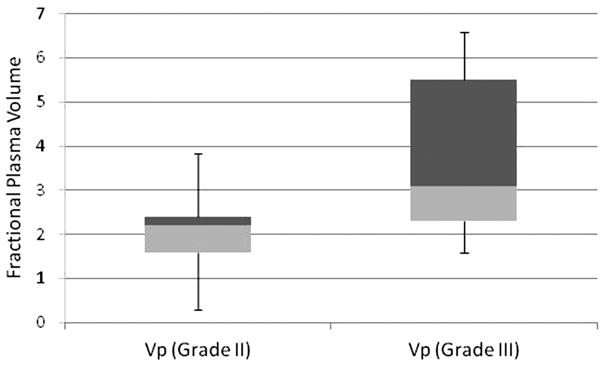
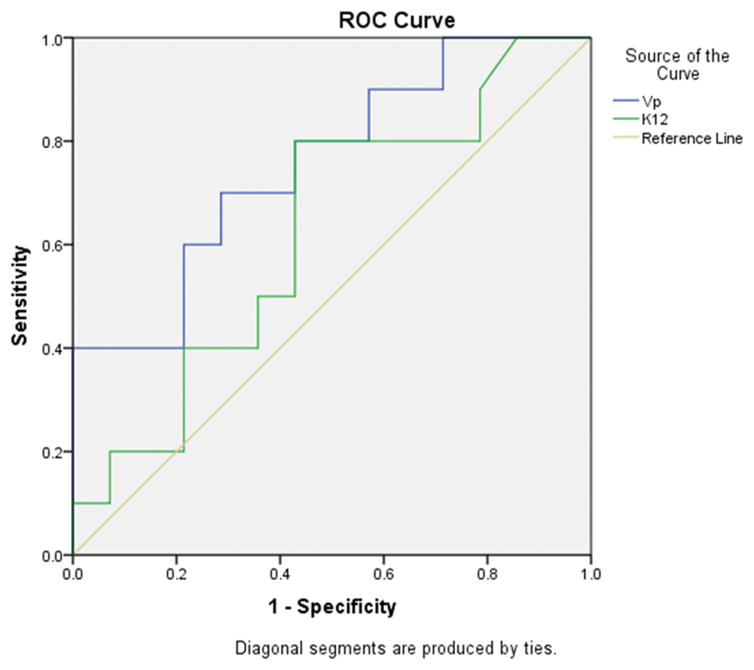
Results: The Vpmean values for grade III oligodendrogliomas were significantly higher (P = .03) than those for grade II oligodendrogliomas. The K(trans) mean values were higher in grade III lesions, but the difference between the 2 groups was not statistically significant (P > .05). Based on ROC analysis, the Vpmean (area under curve = .757, SD = .1) cut-off value that provided the best combination of high sensitivity and specificity to distinguish between grade II and III oligodendrogliomas was 2.35 (P < .03).
Conclusion: The results of our study suggest the DCE MRI parameter Vpmean can noninvasively differentiate between grade II and grade III oligodendrogliomas.
Keywords: DCE; MRI; Oligodendrogliomas.
Copyright © 2015 by the American Society of Neuroimaging.
Figures
References
-
- Bromberg JE, van den Bent MJ. Oligodendrogliomas: molecular biology and treatment. Oncologist. 2009;14:155–63. - PubMed
-
- Le Rhun E, Taillibert S, Chamberlain MC. Anaplastic glioma: current treatment and management. Expert Rev Neurother. 2015;15:601–20. - PubMed
-
- Field M, Witham TF, Flickinger JC, Kondziolka D, Lunsford LD. Comprehensive assessment of hemorrhage risks and outcomes after stereotactic brain biopsy. J Neurosurg. 2001;94:545–51. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
