

A Randomised Comparison Evaluating Changes in Bone Mineral Density in Advanced Prostate Cancer: Luteinising Hormone-releasing Hormone Agonists Versus Transdermal Oestradiol
- PMID: 26707868
- PMCID: PMC4854173
- DOI: 10.1016/j.eururo.2015.11.030
A Randomised Comparison Evaluating Changes in Bone Mineral Density in Advanced Prostate Cancer: Luteinising Hormone-releasing Hormone Agonists Versus Transdermal Oestradiol
Abstract
Background: Luteinising hormone-releasing hormone agonists (LHRHa), used as androgen deprivation therapy (ADT) in prostate cancer (PCa) management, reduce serum oestradiol as well as testosterone, causing bone mineral density (BMD) loss. Transdermal oestradiol is a potential alternative to LHRHa.
Objective: To compare BMD change in men receiving either LHRHa or oestradiol patches (OP).
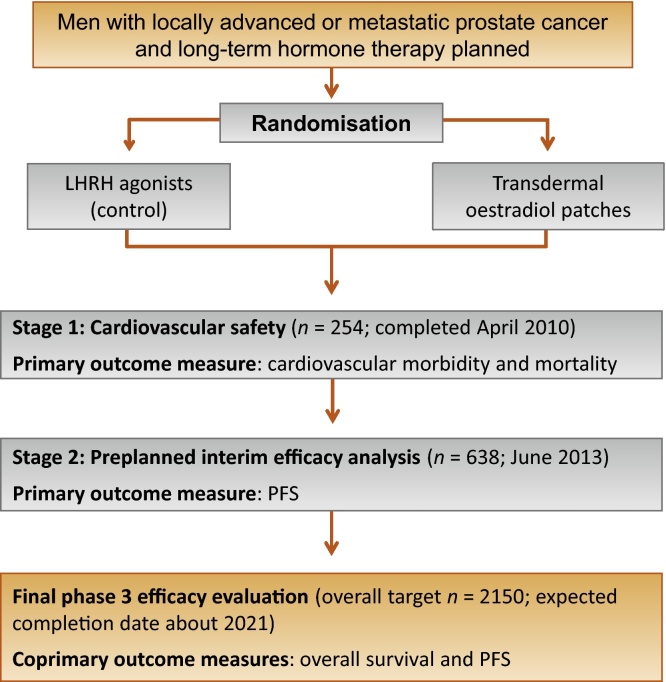
Design, setting, and participants: Men with locally advanced or metastatic PCa participating in the randomised UK Prostate Adenocarcinoma TransCutaneous Hormones (PATCH) trial (allocation ratio of 1:2 for LHRHa:OP, 2006-2011; 1:1, thereafter) were recruited into a BMD study (2006-2012). Dual-energy x-ray absorptiometry scans were performed at baseline, 1 yr, and 2 yr.
Interventions: LHRHa as per local practice, OP (FemSeven 100μg/24h patches).
Outcome measurements and statistical analysis: The primary outcome was 1-yr change in lumbar spine (LS) BMD from baseline compared between randomised arms using analysis of covariance.
Results and limitations: A total of 74 eligible men (LHRHa 28, OP 46) participated from seven centres. Baseline clinical characteristics and 3-mo castration rates (testosterone ≤1.7 nmol/l, LHRHa 96% [26 of 27], OP 96% [43 of 45]) were similar between arms. Mean 1-yr change in LS BMD was -0.021g/cm(3) for patients randomised to the LHRHa arm (mean percentage change -1.4%) and +0.069g/cm(3) for the OP arm (+6.0%; p<0.001). Similar patterns were seen in hip and total body measurements. The largest difference between arms was at 2 yr for those remaining on allocated treatment only: LS BMD mean percentage change LHRHa -3.0% and OP +7.9% (p<0.001).
Conclusions: Transdermal oestradiol as a single agent produces castration levels of testosterone while mitigating BMD loss. These early data provide further supporting evidence for the ongoing phase 3 trial.
Patient summary: This study found that prostate cancer patients treated with transdermal oestradiol for hormonal therapy did not experience the loss in bone mineral density seen with luteinising hormone-releasing hormone agonists. Other clinical outcomes for this treatment approach are being evaluated in the ongoing PATCH trial.
Trial registration: ISRCTN70406718, PATCH trial (ClinicalTrials.gov NCT00303784).
Keywords: Androgen-deprivation therapy; Bone mineral density; Prostate cancer; Transdermal oestradiol.
Copyright © 2015 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures


Comment in
-
Osteoporosis and Fracture Risk in Men with Prostate Cancer.Eur Urol. 2016 Jun;69(6):1026-7. doi: 10.1016/j.eururo.2015.12.036. Epub 2015 Dec 31. Eur Urol. 2016. PMID: 26749094 No abstract available.
References
-
- Diamond T.H., Higano C.S., Smith M.R., Guise T.A., Singer F.R. Osteoporosis in men with prostate carcinoma receiving androgen-deprivation therapy: recommendations for diagnosis and therapies. Cancer. 2004;100:892–899. - PubMed
-
- Morote J., Orsola A., Abascal J.M. Bone mineral density changes in patients with prostate cancer during the first 2 years of androgen suppression. J Urol. 2006;175:1679–1683. discussion 1683. - PubMed
-
- Smith M.R., McGovern F.J., Zietman A.L. Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer. N Engl J Med. 2001;345:948–955. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
