

The Impact of Travel Distance on Breast Reconstruction in the United States
- PMID: 26710002
- PMCID: PMC4776632
- DOI: 10.1097/PRS.0000000000001847
The Impact of Travel Distance on Breast Reconstruction in the United States
Abstract
Background: Inadequate access to breast reconstruction was a motivating factor underlying passage of the Women's Health and Cancer Rights Act. It remains unclear whether all patients interested in breast reconstruction undergo this procedure. The aim of this study was to determine whether geographic disparities are present that limit the rate and method of postmastectomy reconstruction.
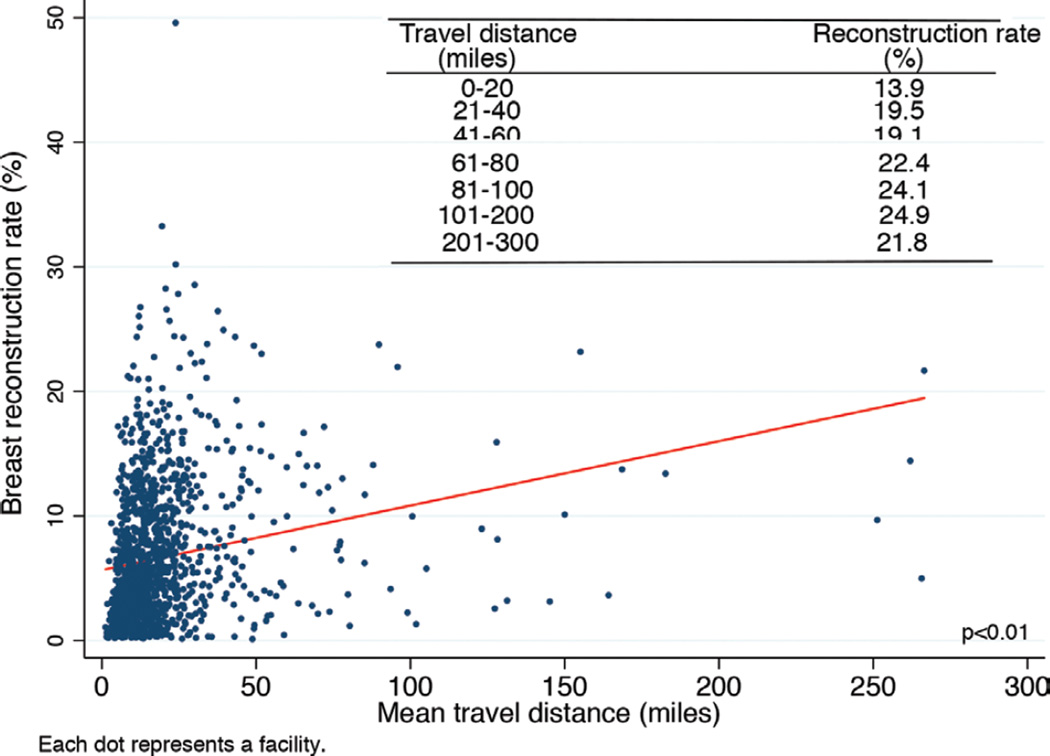
Methods: Travel distance in miles between the patient's residence and the hospital reporting the case was used as a quantitative measure of geographic disparities. The American College of Surgeons National Cancer Database was queried for mastectomy with or without reconstruction performed from 1998 to 2011. Reconstructive procedures were categorized as implant or autologous techniques. Standard statistical tests including linear regression were performed.
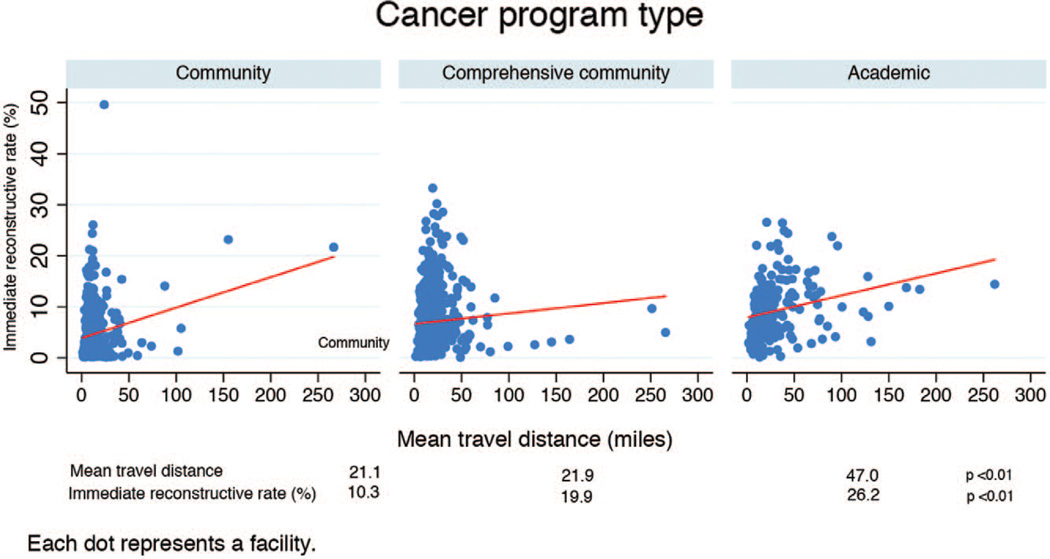
Results: Patients who underwent breast reconstruction had to travel farther than those who had mastectomy alone (p < 0.01). A linear correlation was demonstrated between travel distance and reconstruction rates (p < 0.01). The mean distances traveled by patients who underwent reconstruction at community, comprehensive community, or academic programs were 10.3, 19.9, and 26.2 miles, respectively (p < 0.01). Reconstruction rates were significantly greater at academic programs. Patients traveled farther to undergo autologous compared with prosthetic reconstruction.
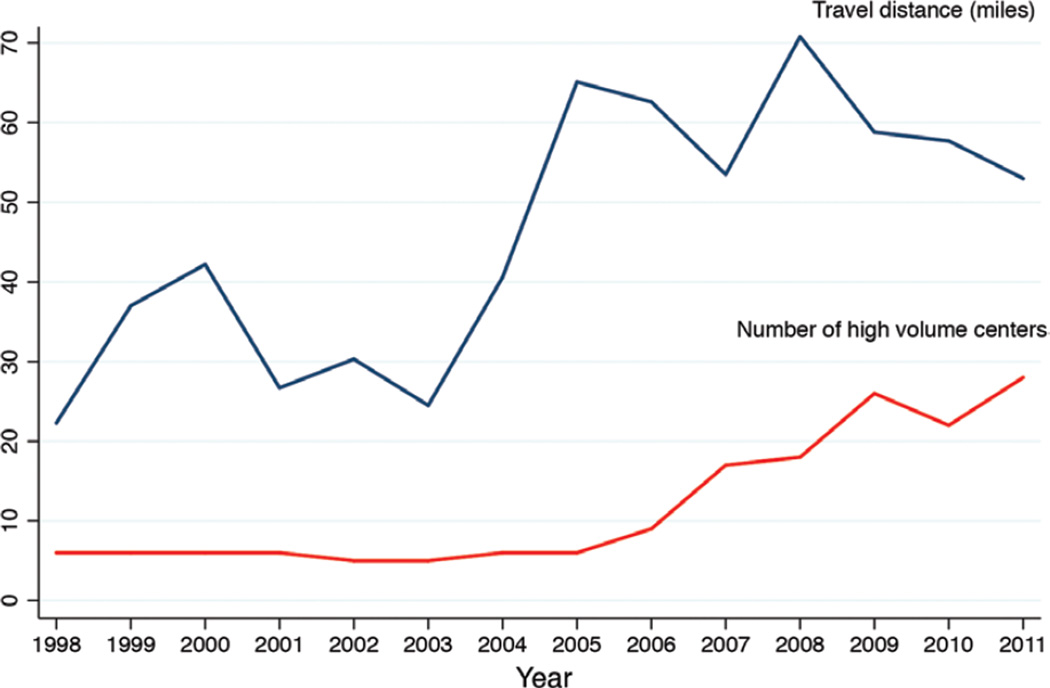
Conclusions: Although greater patient awareness and insurance coverage have contributed to increased breast reconstruction rates in the United States, the presence of geographic barriers suggests an unmet need. Academic programs have the greatest reconstruction rates, but are located farther from patients' residences. Increasing the number of plastics surgeons, especially in community centers, would be one method of addressing this inequality.
Figures
Comment in
-
The Impact of Travel Distance on Breast Reconstruction in the United States.Plast Reconstr Surg. 2016 Aug;138(2):367e. doi: 10.1097/PRS.0000000000002374. Plast Reconstr Surg. 2016. PMID: 27064222 No abstract available.
References
-
- Gulliford M, Figueroa-Munoz J, Morgan M, et al. What does ‘access to health care’ mean? J Health Serv Res Policy. 2002;7:186–188. - PubMed
-
- Women’s Health and Cancer Rights Act of 1998. Available at: http://www.cms.gov/Regulations-and-Guidance/Health-Insurance-Reform/Heal.... Accessed.
-
- Lentol J. Information and Access to Breast Reconstructive Surgery Law. Committee on Codes. Chapter 354; Health. A.10094-B/S.6993-B. Available at: http://assembly.state.ny.us/comm/Codes/2010Annual/index.pdf. Accessed.
-
- Albornoz CR, Bach PB, Pusic AL, et al. The influence of sociodemographic factors and hospital characteristics on the method of breast reconstruction, including microsurgery: A U.S. population-based study. Plast Reconstr Surg. 2012;129:1071–1079. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
