

A State-of-the-Science Overview of Randomized Controlled Trials Evaluating Acute Management of Moderate-to-Severe Traumatic Brain Injury
- PMID: 26711675
- PMCID: PMC5003006
- DOI: 10.1089/neu.2015.4233
A State-of-the-Science Overview of Randomized Controlled Trials Evaluating Acute Management of Moderate-to-Severe Traumatic Brain Injury
Abstract
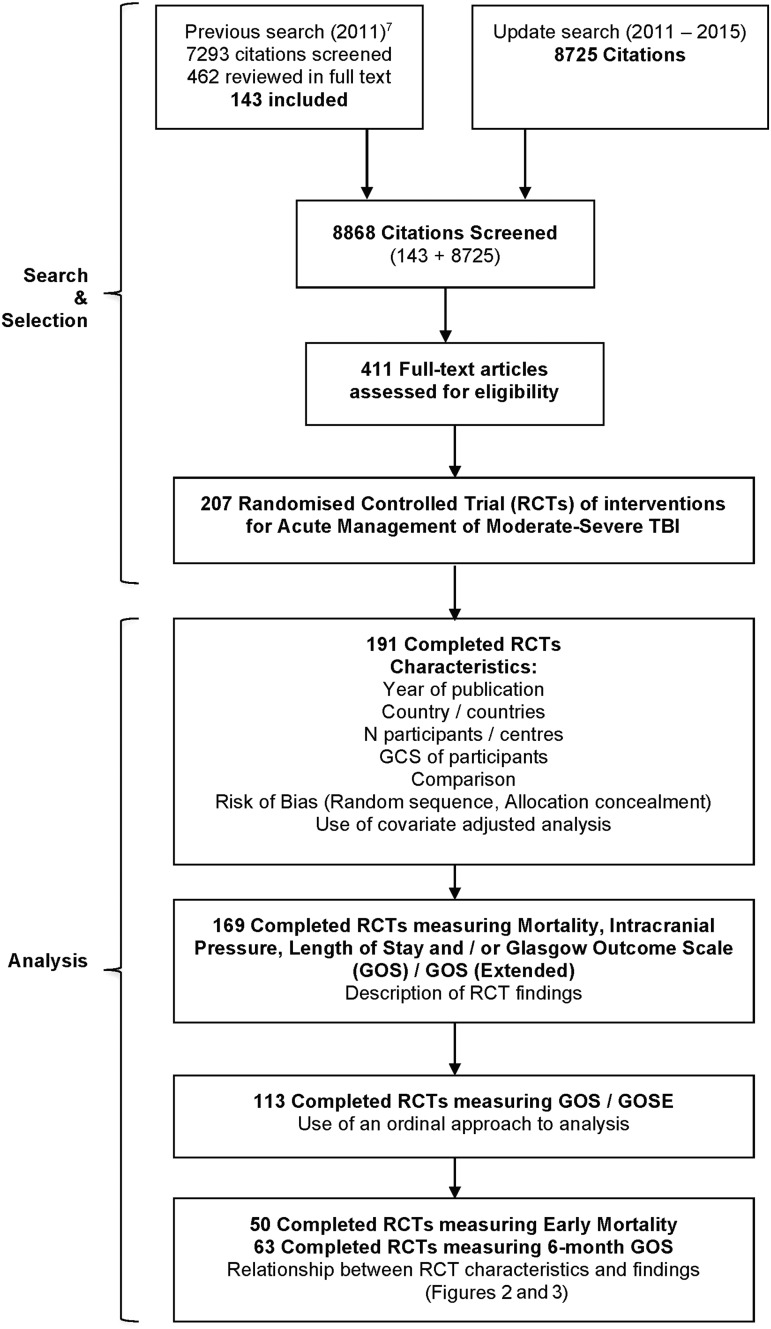
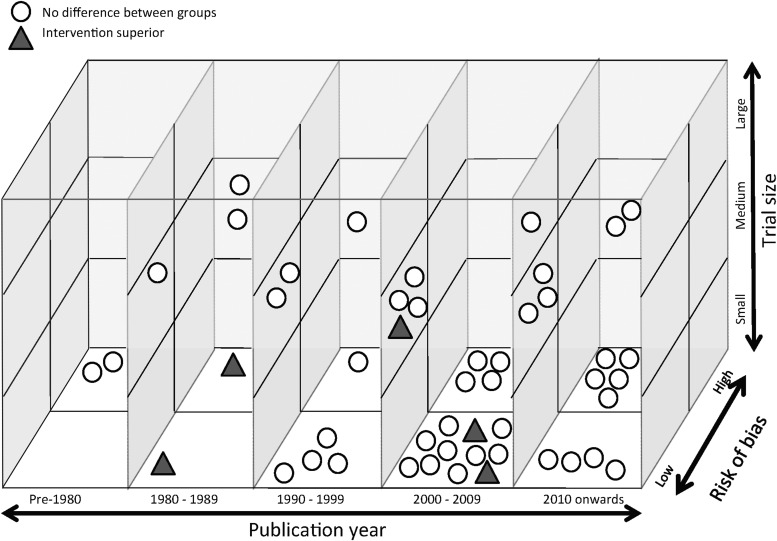
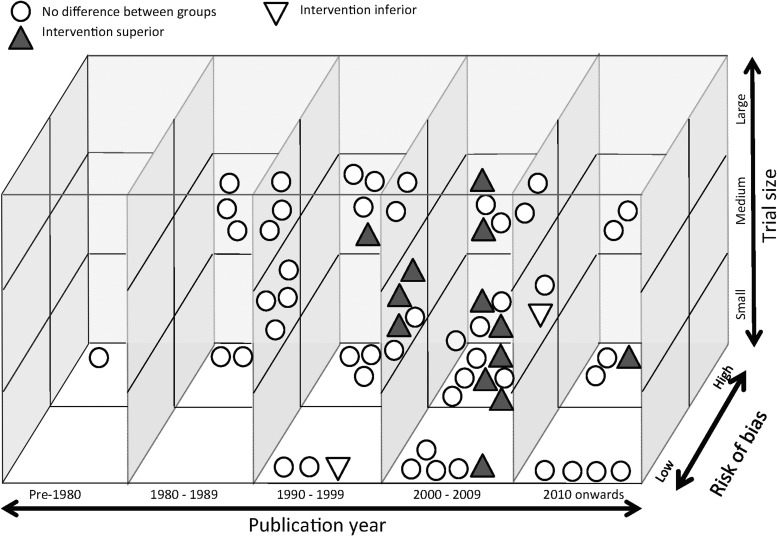
Moderate-to-severe traumatic brain injury (TBI) remains a major global challenge, with rising incidence, unchanging mortality and lifelong impairments. State-of-the-science reviews are important for research planning and clinical decision support. This review aimed to identify randomized controlled trials (RCTs) evaluating interventions for acute management of moderate/severe TBI, synthesize key RCT characteristics and findings, and determine their implications on clinical practice and future research. RCTs were identified through comprehensive database and other searches. Key characteristics, outcomes, risk of bias, and analysis approach were extracted. Data were narratively synthesized, with a focus on robust (multi-center, low risk of bias, n > 100) RCTs, and three-dimensional graphical figures also were used to explore relationships between RCT characteristics and findings. A total of 207 RCTs were identified. The 191 completed RCTs enrolled 35,340 participants (median, 66). Most (72%) were single center and enrolled less than 100 participants (69%). There were 26 robust RCTs across 18 different interventions. For 74% of 392 comparisons across all included RCTs, there was no significant difference between groups. Positive findings were broadly distributed with respect to RCT characteristics. Less than one-third of RCTs demonstrated low risk of bias for random sequence generation or allocation concealment, less than one-quarter used covariate adjustment, and only 7% employed an ordinal analysis approach. Considerable investment of resources in producing 191 completed RCTs for acute TBI management has resulted in very little translatable evidence. This may result from broad distribution of research effort, small samples, preponderance of single-center RCTs, and methodological shortcomings. More sophisticated RCT design, large multi-center RCTs in priority areas, increased focus on pre-clinical research, and alternatives to RCTs, such as comparative effectiveness research and precision medicine, are needed to fully realize the potential of acute TBI research to benefit patients.
Keywords: clinical trial; review; traumatic brain injury.
Figures
References
-
- Abelson-Mitchell N. (2008). Epidemiology and prevention of head injuries: literature review. J. Clin. Nurs. 17, 46–57 - PubMed
-
- Roozenbeek B., Maas A.I., and Menon D.K. (2013). Changing patterns in the epidemiology of traumatic brain injury. Nat. Rev. Neurol. 9, 231–236 - PubMed
-
- Feigin V.L., Theadom A., Barker-Collo S., Starkey N.J., McPherson K., Kahan M., Dowell A., Brown P., Parag V., Kydd R., Jones K., Jones A., and Ameratunga S; BIONIC Study Group. (2013). Incidence of traumatic brain injury in New Zealand: a population-based study. Lancet Neurol. 12, 53–64 - PubMed
-
- Maas A.I., Stocchetti N., and Bullock R. (2008). Moderate and severe traumatic brain injury in adults. Lancet Neurol. 7, 728–741 - PubMed
-
- Khan F., Baguley I.J., and Cameron I.D. (2003). 4: Rehabilitation after traumatic brain injury. Med. J. Aust. 178, 290–295 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
