

Prevalence and Prognostic Significance of Apparent Treatment Resistant Hypertension in Chronic Kidney Disease: Report From the Chronic Renal Insufficiency Cohort Study
- PMID: 26711738
- PMCID: PMC4713320
- DOI: 10.1161/HYPERTENSIONAHA.115.06487
Prevalence and Prognostic Significance of Apparent Treatment Resistant Hypertension in Chronic Kidney Disease: Report From the Chronic Renal Insufficiency Cohort Study
Abstract
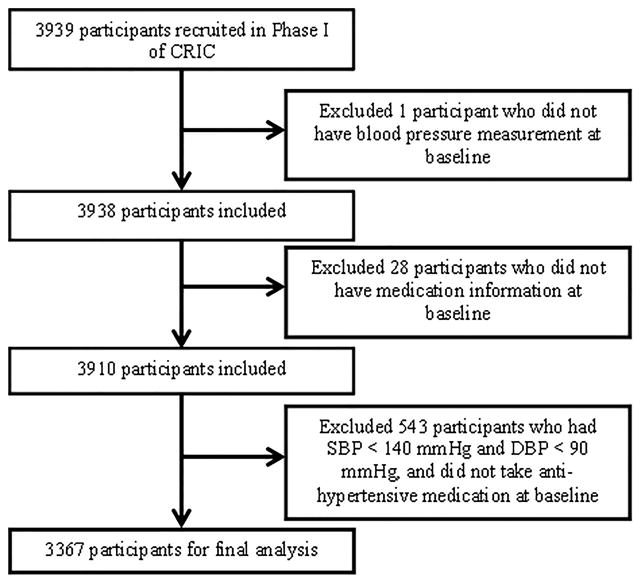
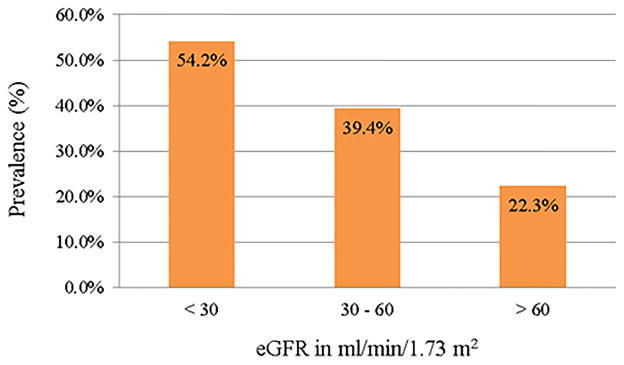
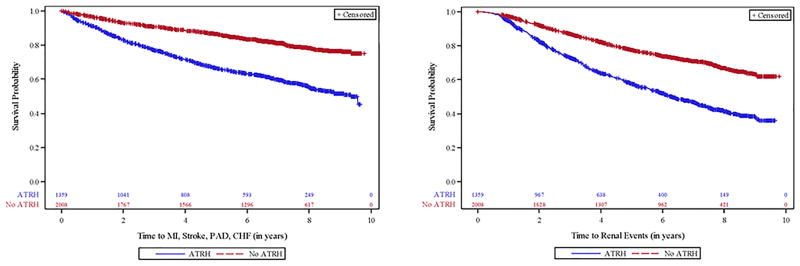
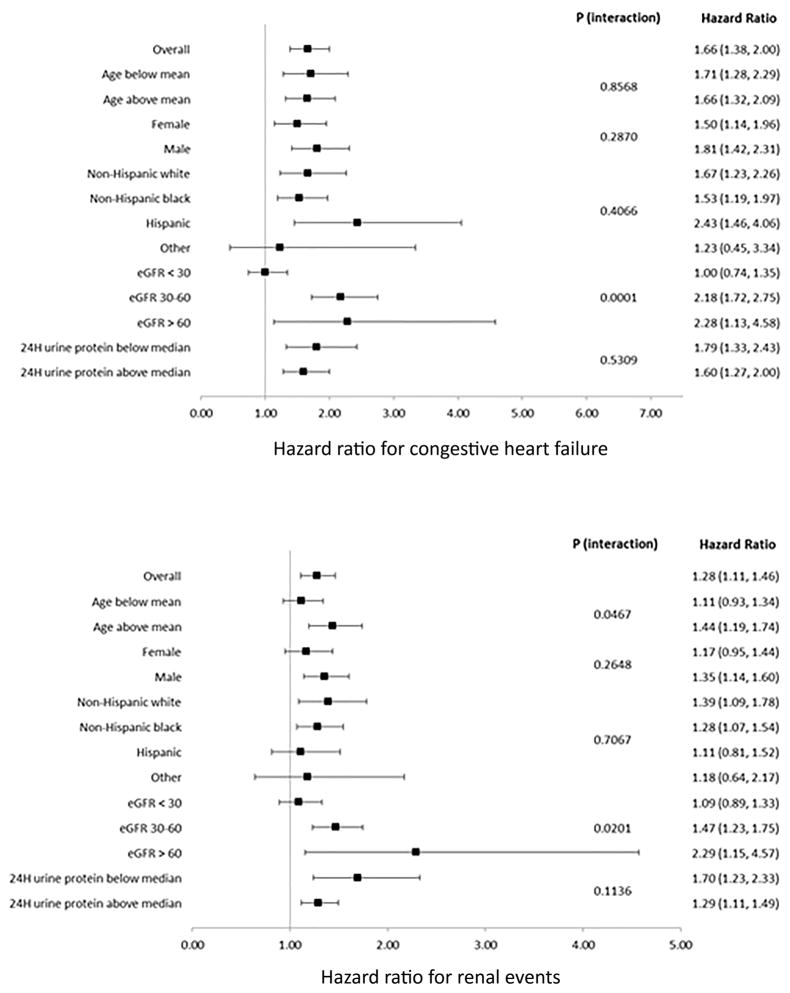
The association between apparent treatment resistant hypertension (ATRH) and clinical outcomes is not well studied in chronic kidney disease. We analyzed data on 3367 hypertensive participants in the Chronic Renal Insufficiency Cohort (CRIC) to determine prevalence, associations, and clinical outcomes of ATRH in nondialysis chronic kidney disease patients. ATRH was defined as blood pressure ≥140/90 mm Hg on ≥3 antihypertensives, or use of ≥4 antihypertensives with blood pressure at goal at baseline visit. Prevalence of ATRH was 40.4%. Older age, male sex, black race, diabetes mellitus, and higher body mass index were independently associated with higher odds of having ATRH. Participants with ATRH had a higher risk of clinical events than participants without ATRH-composite of myocardial infarction, stroke, peripheral arterial disease, congestive heart failure (CHF), and all-cause mortality (hazard ratio [95% confidence interval], 1.38 [1.22-1.56]); renal events (1.28 [1.11-1.46]); CHF (1.66 [1.38-2.00]); and all-cause mortality (1.24 [1.06-1.45]). The subset of participants with ATRH and blood pressure at goal on ≥4 medications also had higher risk for composite of myocardial infarction, stroke, peripheral arterial disease, CHF, and all-cause mortality (hazard ratio [95% confidence interval], (1.30 [1.12-1.51]) and CHF (1.59 [1.28-1.99]) than those without ATRH. ATRH was associated with significantly higher risk for CHF and renal events only among those with estimated glomerular filtration rate ≥30 mL/min per 1.73 m(2). Our findings show that ATRH is common and associated with high risk of adverse outcomes in a cohort of patients with chronic kidney disease. This underscores the need for early identification and management of patients with ATRH and chronic kidney disease.
Keywords: antihypertensive agents; hypertension; hypertension resistant to conventional therapy; myocardial infarction; renal insufficiency, chronic.
© 2015 American Heart Association, Inc.
Conflict of interest statement
Conflict(s) of Interest/Disclosure(s)
John M. Flack: The Medicines Company (consultant), Medtronic (consultant and member of the steering committee for SYMPLICITY HTN 3), BackBeat Medical, Inc. (consultant)
Raymond R. Townsend: Medtronic (consultant)
Figures
Comment in
-
Obesity, African American Race, Chronic Kidney Disease, and Resistant Hypertension: The Step Beyond Observed Risk.Hypertension. 2016 Feb;67(2):275-7. doi: 10.1161/HYPERTENSIONAHA.115.06563. Epub 2015 Dec 28. Hypertension. 2016. PMID: 26711736 Free PMC article. No abstract available.
References
-
- Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, White A, Cushman WC, White W, Sica D, Ferdinand K, Giles TD, Falkner B, Carey RM. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403–1419. - PubMed
-
- Persell SD. Prevalence of resistant hypertension in the United States, 2003–2008. Hypertension. 2011;57:1076–1080. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01DK060963/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 RR-024131/RR/NCRR NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR-000424/TR/NCATS NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1 TR000114/TR/NCATS NIH HHS/United States
- U01DK060980/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- U01DK061021/DK/NIDDK NIH HHS/United States
- P30GM103337/GM/NIGMS NIH HHS/United States
- U01DK060984/DK/NIDDK NIH HHS/United States
- UL1RR029879/RR/NCRR NIH HHS/United States
- U01DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- U01DK061028/DK/NIDDK NIH HHS/United States
- UL1TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- U01DK060902/DK/NIDDK NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- M01 RR-16500/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
