

Posttreatment Antifungal Resistance among Colonizing Candida Isolates in Candidemia Patients: Results from a Systematic Multicenter Study
- PMID: 26711776
- PMCID: PMC4775986
- DOI: 10.1128/AAC.01763-15
Posttreatment Antifungal Resistance among Colonizing Candida Isolates in Candidemia Patients: Results from a Systematic Multicenter Study
Abstract
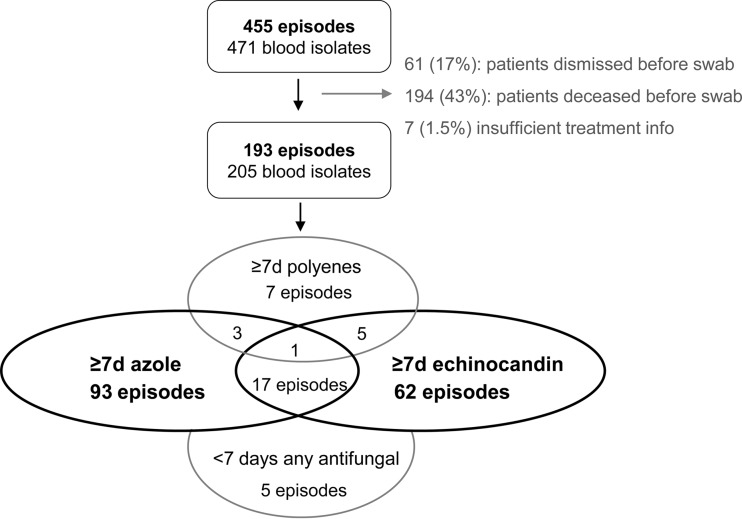
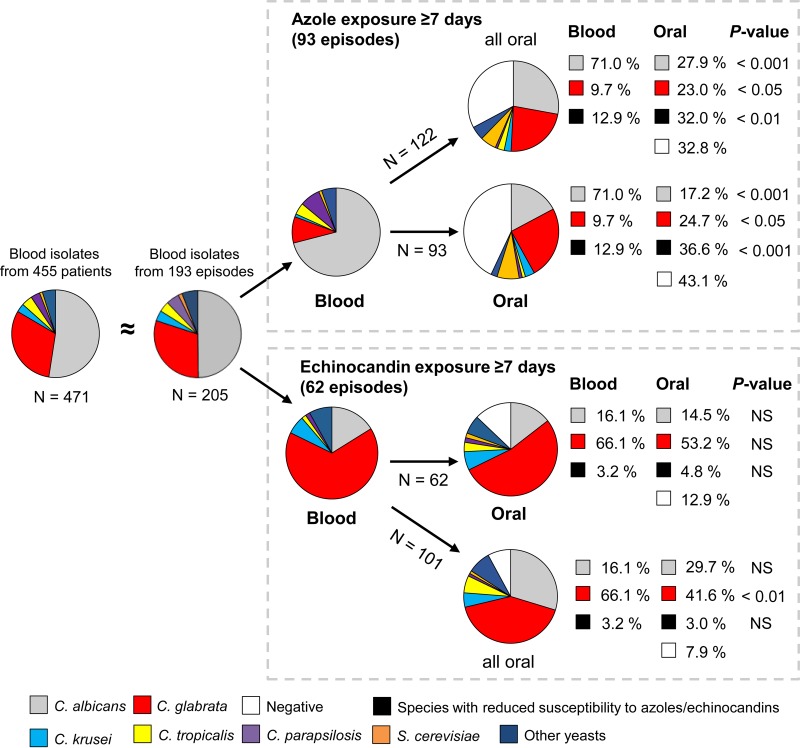
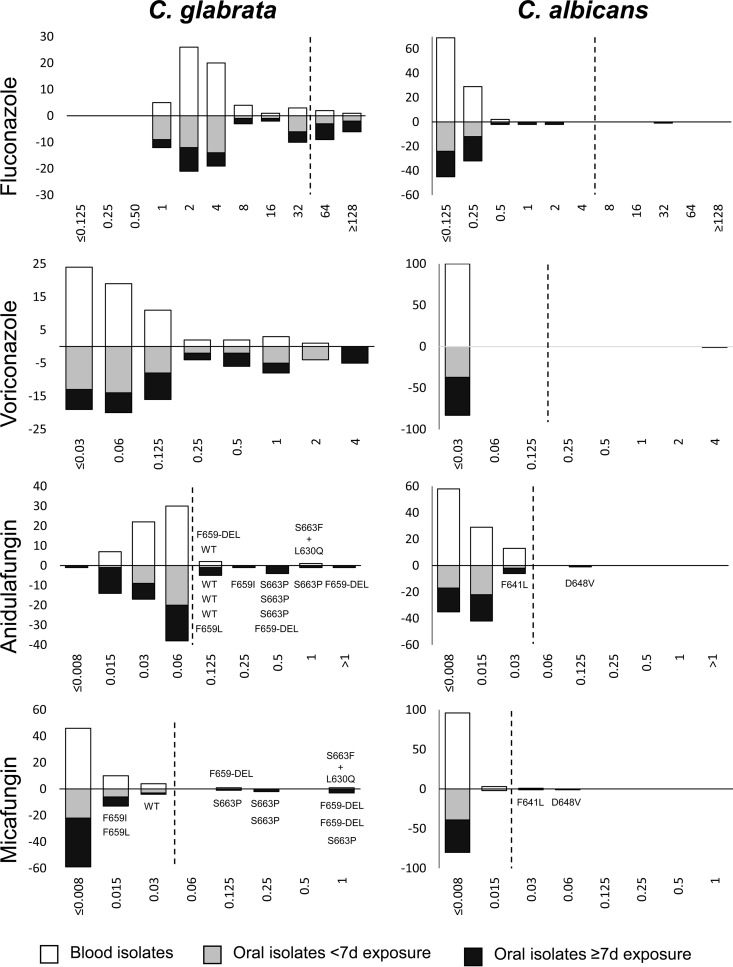
The prevalence of intrinsic and acquired resistance among colonizing Candida isolates from patients after candidemia was investigated systematically in a 1-year nationwide study. Patients were treated at the discretion of the treating physician. Oral swabs were obtained after treatment. Species distributions and MIC data were investigated for blood and posttreatment oral isolates from patients exposed to either azoles or echinocandins for <7 or ≥ 7 days. Species identification was confirmed using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) and internal transcribed spacer (ITS) sequencing, susceptibility was examined by EUCAST EDef 7.2 methodology, echinocandin resistance was examined by FKS sequencing, and genetic relatedness was examined by multilocus sequence typing (MLST). One hundred ninety-three episodes provided 205 blood and 220 oral isolates. MLST analysis demonstrated a genetic relationship for 90% of all paired blood and oral isolates. Patients exposed to azoles for ≥ 7 days (n = 93) had a significantly larger proportion of species intrinsically less susceptible to azoles (particularly Candida glabrata) among oral isolates than among initial blood isolates (36.6% versus 12.9%; P < 0.001). A similar shift toward species less susceptible to echinocandins among 85 patients exposed to echinocandins for ≥ 7 days was not observed (4.8% of oral isolates versus 3.2% of blood isolates; P > 0.5). Acquired resistance in Candida albicans was rare (<5%). However, acquired resistance to fluconazole (29.4%; P < 0.05) and anidulafungin (21.6%; P < 0.05) was common in C. glabrata isolates from patients exposed to either azoles or echinocandins. Our findings suggest that the colonizing mucosal microbiota may be an unrecognized reservoir of resistant Candida species, especially C. glabrata, following treatment for candidemia. The resistance rates were high, raising concern in general for patients exposed to antifungal drugs.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Arendrup MC, Dzajic E, Jensen RH, Johansen HK, Kjaeldgaard P, Knudsen JD, Kristensen L, Leitz C, Lemming LE, Nielsen L, Olesen B, Rosenvinge FS, Røder BL, Schønheyder HC. 2013. Epidemiological changes with potential implication for antifungal prescription recommendations for fungaemia: data from a nationwide fungaemia surveillance programme. Clin Microbiol Infect 19:E343–E353. doi:10.1111/1469-0691.12212. - DOI - PubMed
-
- Tortorano AM, Prigitano A, Lazzarini C, Passera M, Deiana ML, Cavinato S, De Luca C, Grancini A, Lo Cascio G, Ossi C, Sala E, Montagna MT. 2013. A 1-year prospective survey of candidemia in Italy and changing epidemiology over one decade. Infection 41:655–662. doi:10.1007/s15010-013-0455-6. - DOI - PubMed
-
- Lockhart SR, Iqbal N, Cleveland AA, Farley MM, Harrison LH, Bolden CB, Baughman W, Stein B, Hollick R, Park BJ, Chiller T. 2012. Species identification and antifungal susceptibility testing of Candida bloodstream isolates from population-based surveillance studies in two U.S. cities from 2008 to 2011. J Clin Microbiol 50:3435–3442. doi:10.1128/JCM.01283-12. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
