

Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites
- PMID: 26712231
- PMCID: PMC4872030
- DOI: 10.1200/JCO.2015.64.0987
Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites
Abstract
Purpose: Gastro-entero-pancreatic neuroendocrine tumors (GEPNETs) are increasing in incidence, and accurate staging is important for selecting the appropriate treatment. (68)Ga-DOTATATE imaging is a promising approach for detecting GEPNETs and could help in selecting optimal therapeutic strategies. The aim of this study was to prospectively determine the clinical utility of (68)Ga-DOTATATE positron emission tomography (PET)/computed tomography (CT) in detecting unknown primary and metastatic GEPNETs.
Patients and methods: One hundred thirty-one patients were enrolled in a prospective study of patients undergoing (68)Ga-DOTATATE PET/CT, (111)In-pentetreotide single-photon emission computed tomography (SPECT)/CT and multiphasic CT scan, and/or magnetic resonance imaging in a blinded fashion with comprehensive biochemical testing. The primary outcome measure was the detection of lesions by each imaging study.
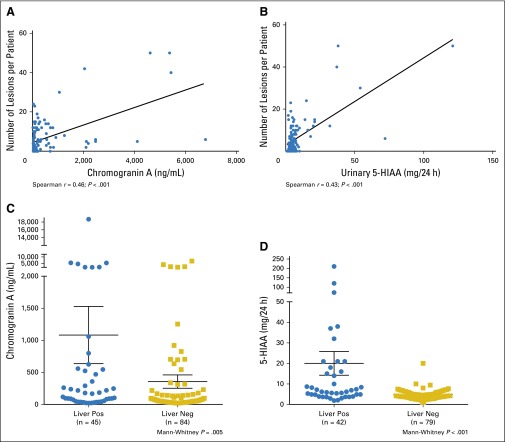
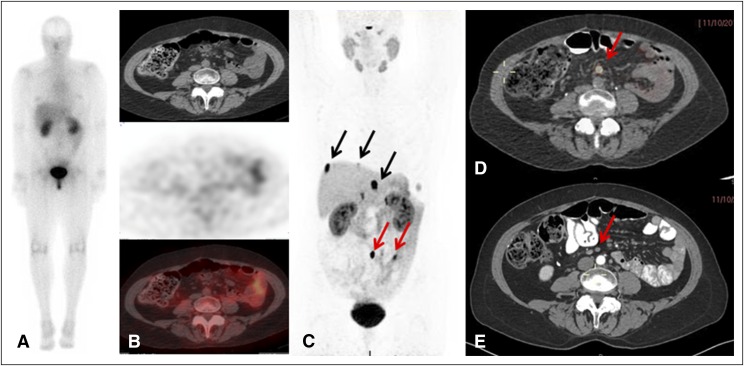
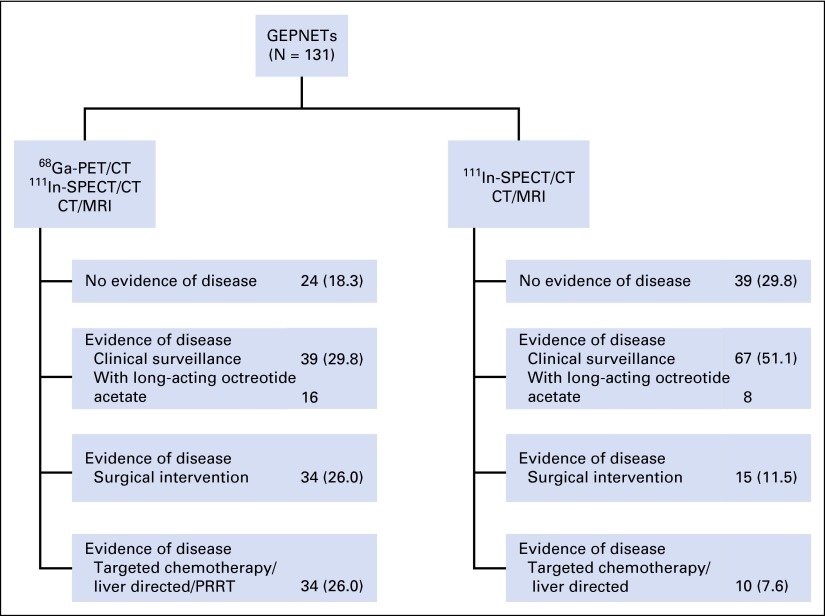
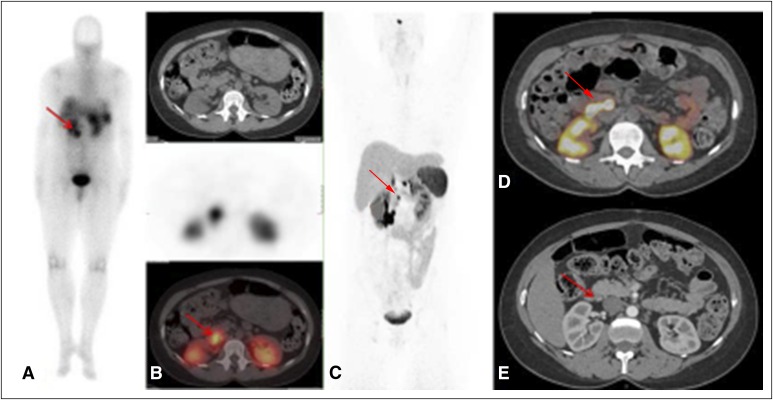
Results: (68)Ga-DOTATATE PET/CT imaging detected 95.1% of lesions (95% CI, 92.4% to 96.8%) with an average maximum standardized uptake value of 65.4 ± 47 (range, 6.9 to 244), anatomic imaging detected 45.3% of lesions (95% CI, 37.9% to 52.9%), and (111)In-pentetreotide SPECT/CT detected 30.9% of lesions (95% CI, 25.0% to 37.5%), with a significant difference between imaging modalities (P < .001). In four of 14 patients (28.6%), (68)Ga-DOTATATE PET/CT found a previously unknown primary tumor, and detected primary GEPNET, lymph node, and distant metastases correctly in 72 of 113 lesions (63.7%) when compared with histopathology, with 22.1% and 38.9% detected by using (111)In-pentetreotide SPECT/CT and anatomic imaging, respectively. On the basis of findings with (68)Ga-DOTATATE PET/CT, 43 of 131 patients (32.8%) had a change in management recommendation. In patients with carcinoid symptoms but negative biochemical testing, (68)Ga-DOTATATE PET/CT detected lesions in 65.2% of patients, 40% of which were detected neither by anatomic imaging nor by (111)In-pentetreotide SPECT/CT.
Conclusion: (68)Ga-DOTATATE PET/CT imaging provides important information for accurate staging of GEPNETs and selection of appropriate treatment interventions even in the absence of biochemical evidence of disease in symptomatic patients.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Similar articles
-
Can complementary 68Ga-DOTATATE and 18F-FDG PET/CT establish the missing link between histopathology and therapeutic approach in gastroenteropancreatic neuroendocrine tumors?J Nucl Med. 2014 Nov;55(11):1811-7. doi: 10.2967/jnumed.114.142224. Epub 2014 Oct 14. J Nucl Med. 2014. PMID: 25315243
-
Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors.J Nucl Med. 2016 May;57(5):708-14. doi: 10.2967/jnumed.115.163865. Epub 2016 Jan 14. J Nucl Med. 2016. PMID: 26769865 Free PMC article.
-
MIB-1 Index-Stratified Assessment of Dual-Tracer PET/CT with 68Ga-DOTATATE and 18F-FDG and Multimodality Anatomic Imaging in Metastatic Neuroendocrine Tumors of Unknown Primary in a PRRT Workup Setting.J Nucl Med Technol. 2017 Mar;45(1):34-41. doi: 10.2967/jnmt.116.185777. Epub 2017 Feb 2. J Nucl Med Technol. 2017. PMID: 28154019
-
Cardiac neuroendocrine tumour metastases: case reports and review of the literature.Nucl Med Commun. 2016 May;37(5):461-5. doi: 10.1097/MNM.0000000000000464. Nucl Med Commun. 2016. PMID: 26671851 Review.
-
Gastro-Entero-Pancreatic Tumors: FDG Positron Emission Tomography/Computed Tomography.PET Clin. 2023 Apr;18(2):243-250. doi: 10.1016/j.cpet.2022.11.007. Epub 2023 Jan 25. PET Clin. 2023. PMID: 36707371 Review.
Cited by
-
Role of Somatostatin Receptor in Pancreatic Neuroendocrine Tumor Development, Diagnosis, and Therapy.Front Endocrinol (Lausanne). 2021 May 19;12:679000. doi: 10.3389/fendo.2021.679000. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34093445 Free PMC article. Review.
-
Evaluation of 18F-AlF-NOTA-octreotide for imaging neuroendocrine neoplasms: comparison with 68Ga-DOTATATE PET/CT.EJNMMI Res. 2021 Jun 9;11(1):55. doi: 10.1186/s13550-021-00797-4. EJNMMI Res. 2021. PMID: 34106351 Free PMC article.
-
A combination of surgery, theranostics, and liquid biopsy - a personalised oncologic approach to treatment of patients with advanced metastatic neuroendocrine neoplasms.Int J Med Sci. 2021 Mar 19;18(10):2166-2175. doi: 10.7150/ijms.51740. eCollection 2021. Int J Med Sci. 2021. PMID: 33859524 Free PMC article.
-
Somatostatinoma and Neurofibromatosis Type 1-A Case Report and Review of the Literature.Diagnostics (Basel). 2020 Aug 21;10(9):620. doi: 10.3390/diagnostics10090620. Diagnostics (Basel). 2020. PMID: 32825782 Free PMC article.
-
Evolving landscape of clinical trials in gastroenteropancreatic neuroendocrine neoplasms in the past two decades.Endocr Connect. 2023 Mar 10;12(4):e220441. doi: 10.1530/EC-22-0441. Print 2023 Apr 1. Endocr Connect. 2023. PMID: 36724047 Free PMC article.
References
-
- Lawrence B, Gustafsson BI, Chan A, et al. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. 2011;40:1–18. doi:10.1016/j.ecl.2010.12.005. - PubMed
-
- Duh QY, Hybarger CP, Geist R, et al. Carcinoids associated with multiple endocrine neoplasia syndromes. Am J Surg. 1987;154:142–148. - PubMed
-
- Charlesworth M, Verbeke CS, Falk GA, et al. Pancreatic lesions in von Hippel-Lindau disease? A systematic review and meta-synthesis of the literature. J Gastrointest Surg. 2012;16:1422–1428. - PubMed
-
- Larson AM, Hedgire SS, Deshpande V, et al. Pancreatic neuroendocrine tumors in patients with tuberous sclerosis complex. Clin Genet. 2012;82:558–563. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
