

Micro-CT in the Assessment of Pediatric Renal Osteodystrophy by Bone Histomorphometry
- PMID: 26712809
- PMCID: PMC4791816
- DOI: 10.2215/CJN.04810515
Micro-CT in the Assessment of Pediatric Renal Osteodystrophy by Bone Histomorphometry
Abstract
Background and objectives: Computed tomography (CT) measurements can distinguish between cortical and trabecular bone density in vivo. High-resolution CTs assess both bone volume and density in the same compartment, thus potentially yielding information regarding bone mineralization as well. The relationship between bone histomorphometric parameters of skeletal mineralization and bone density from microcomputed tomography (μCT) measurements of bone cores from patients on dialysis has not been assessed.
Design, setting, participants, & measurements: Bone cores from 68 patients with ESRD (age =13.9±0.5 years old; 50% men) and 14 controls (age =15.3±3.8 years old; 50% men) obtained as part of research protocols between 1983 and 2006 were analyzed by bone histomorphometry and μCT.
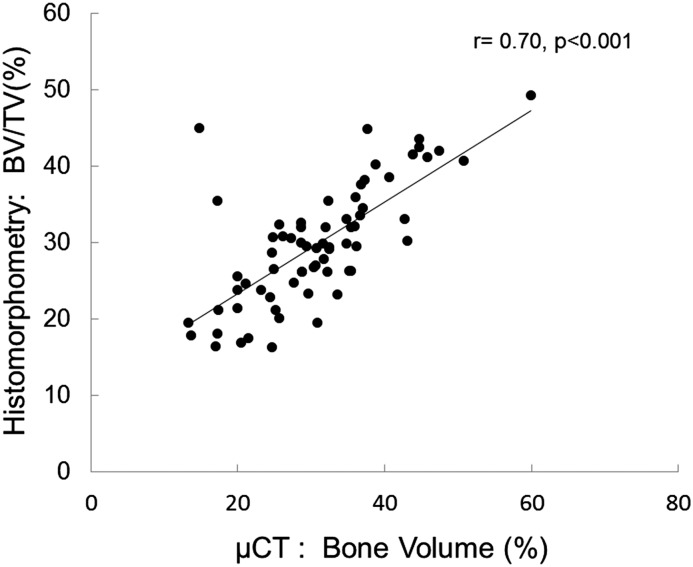
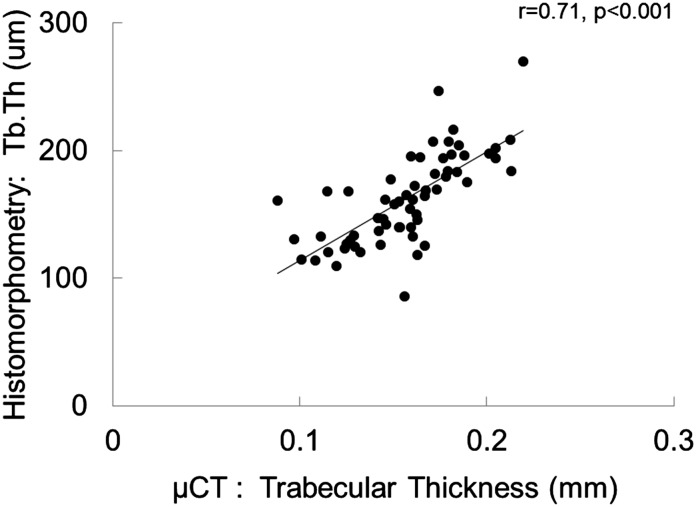
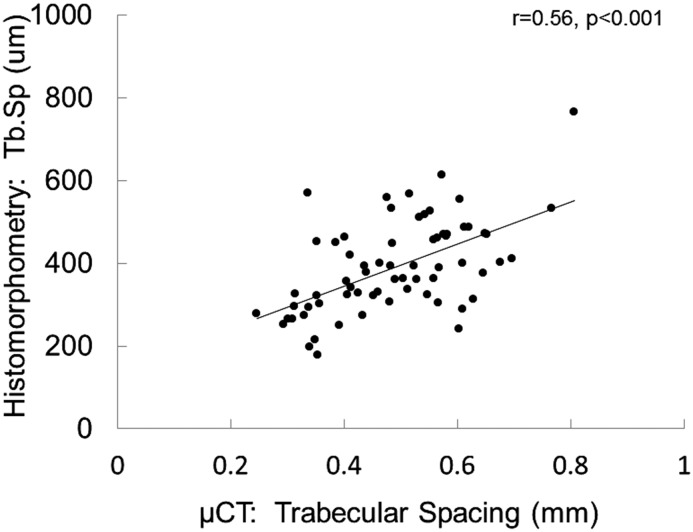
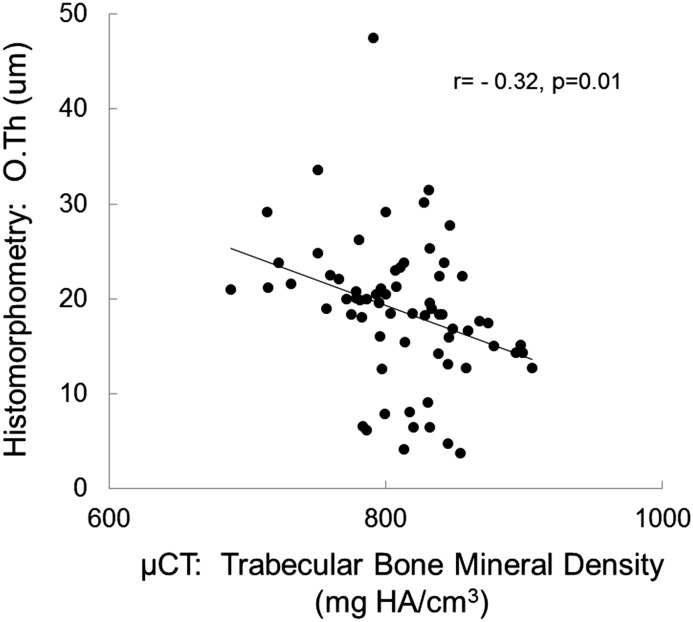
Results: Bone histomorphometric diagnoses in the patients were normal to high bone turnover in 76%, adynamic bone in 13%, and osteomalacia in 11%. Bone formation rate did not correlate with any μCT determinations. Bone volume measurements were highly correlated between bone histomorphometry and μCT (bone volume/tissue volume between the two techniques: r=0.70; P<0.001, trabecular thickness and trabecular separation: r=0.71; P<0.001, and r=0.56; P<0.001, respectively). Osteoid accumulation as determined by bone histomorphometry correlated inversely with bone mineral density as assessed by μCT (osteoid thickness: r=-0.32; P=0.01 and osteoid volume: r=-0.28; P=0.05). By multivariable analysis, the combination of bone mineral density and bone volume (as assessed by μCT) along with parathyroid hormone and calcium levels accounted for 38% of the variability in osteoid volume (by histomorphometry).
Conclusions: Measures of bone volume can be accurately assessed with μCT. Bone mineral density is lower in patients with excessive osteoid accumulation and higher in patients with adynamic, well mineralized bone. Thus, bone mineralization may be accurately assessed by μCT of bone biopsy cores. Additional studies are warranted to define the value of high-resolution CT in the prediction of bone mineralization in vivo.
Keywords: bone biopsy; bone density; calcification, physiologic; child; humans; kidney failure, chronic; micro CT; renal dialysis; renal osteodystrophy.
Copyright © 2016 by the American Society of Nephrology.
Figures
Similar articles
-
Can bone histomorphometry be predicted by clinical assessment and noninvasive techniques in peritoneal dialysis?Miner Electrolyte Metab. 1996;22(4):224-33. Miner Electrolyte Metab. 1996. PMID: 8807626
-
Changes in Bone Histomorphometry after Kidney Transplantation.Clin J Am Soc Nephrol. 2019 Jun 7;14(6):894-903. doi: 10.2215/CJN.09950818. Epub 2019 May 14. Clin J Am Soc Nephrol. 2019. PMID: 31088851 Free PMC article.
-
Renal osteodystrophy: alpha-Heremans Schmid glycoprotein/fetuin-A, matrix GLA protein serum levels, and bone histomorphometry.Am J Kidney Dis. 2006 Jul;48(1):106-13. doi: 10.1053/j.ajkd.2006.03.083. Am J Kidney Dis. 2006. PMID: 16797392
-
Bone histomorphometry in renal osteodystrophy.Semin Nephrol. 2009 Mar;29(2):122-32. doi: 10.1016/j.semnephrol.2009.01.005. Semin Nephrol. 2009. PMID: 19371803 Review.
-
Renal bone disease: a new conceptual framework for the interpretation of bone histomorphometry.Curr Opin Nephrol Hypertens. 2003 Jul;12(4):387-403. doi: 10.1097/00041552-200307000-00007. Curr Opin Nephrol Hypertens. 2003. PMID: 12815335 Review.
Cited by
-
Regulation of osteoblast behaviors via cross-talk between Hippo/YAP and MAPK signaling pathway under fluoride exposure.J Mol Med (Berl). 2019 Jul;97(7):1003-1017. doi: 10.1007/s00109-019-01785-x. Epub 2019 May 4. J Mol Med (Berl). 2019. PMID: 31055605
-
Correlations between radiological and histological findings of bone remodelling and root resorption in a rodent cleft model.Head Face Med. 2022 Nov 11;18(1):33. doi: 10.1186/s13005-022-00338-x. Head Face Med. 2022. PMID: 36357936 Free PMC article.
-
Proportional vascularization along the fallopian tubes and ovarian fimbria: assessment by confocal microtomography.Radiol Bras. 2020 May-Jun;53(3):161-166. doi: 10.1590/0100-3984.2019.0080. Radiol Bras. 2020. PMID: 32587423 Free PMC article.
-
Canadian Society of Nephrology Commentary on the Kidney Disease Improving Global Outcomes 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder.Can J Kidney Health Dis. 2020 Aug 4;7:2054358120944271. doi: 10.1177/2054358120944271. eCollection 2020. Can J Kidney Health Dis. 2020. PMID: 32821415 Free PMC article.
-
Bone Fragility Fractures in CKD Patients.Calcif Tissue Int. 2021 Apr;108(4):539-550. doi: 10.1007/s00223-020-00779-z. Epub 2020 Nov 21. Calcif Tissue Int. 2021. PMID: 33219822 Free PMC article. Review.
References
-
- Jamal SA, West SL, Nickolas TL: The clinical utility of FRAX to discriminate fracture status in men and women with chronic kidney disease. Osteoporos Int 25: 71–76, 2014 - PubMed
-
- Groothoff JW, Offringa M, Van Eck-Smit BL, Gruppen MP, Van De Kar NJ, Wolff ED, Lilien MR, Davin JC, Heymans HS, Dekker FW: Severe bone disease and low bone mineral density after juvenile renal failure. Kidney Int 63: 266–275, 2003 - PubMed
-
- Moe S, Drüeke T, Cunningham J, Goodman W, Martin K, Olgaard K, Ott S, Sprague S, Lameire N, Eknoyan G, Kidney Disease: Improving Global Outcomes (KDIGO) : Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 69: 1945–1953, 2006 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group: KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 113:S1-130, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
