

Cost-Utility Analysis of a Cardiac Telerehabilitation Program: The Teledialog Project
- PMID: 26713491
- PMCID: PMC4939376
- DOI: 10.1089/tmj.2015.0194
Cost-Utility Analysis of a Cardiac Telerehabilitation Program: The Teledialog Project
Abstract
Background: Cardiac rehabilitation can reduce mortality of patients with cardiovascular disease, but a frequently low participation rate in rehabilitation programs has been found globally. The objective of the Teledialog study was to assess the cost-utility (CU) of a cardiac telerehabilitation (CTR) program. The aim of the intervention was to increase the patients' participation in the CTR program. At discharge, an individualized 3-month rehabilitation plan was formulated for each patient. At home, the patients measured their own blood pressure, pulse, weight, and steps taken for 3 months.
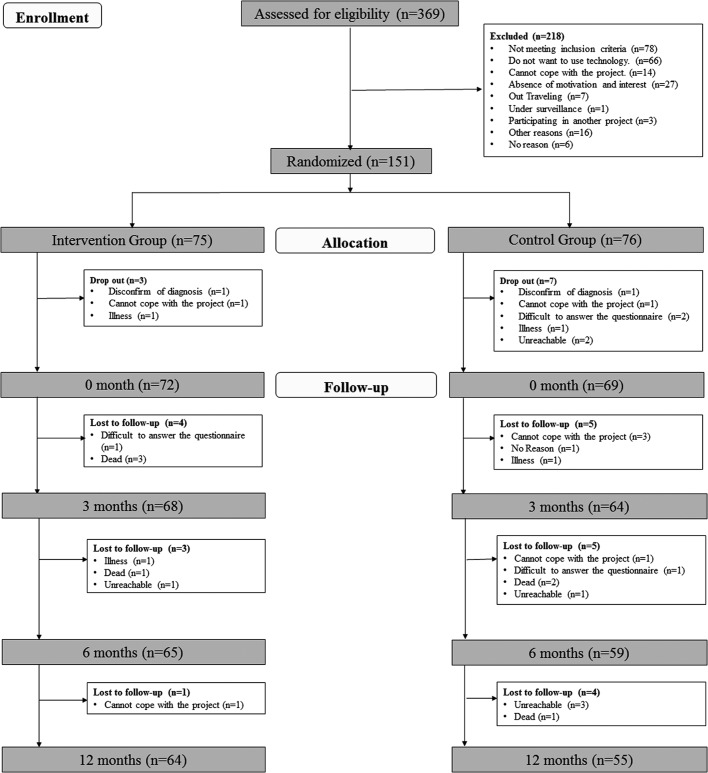
Materials and methods: The analysis was carried out together with a randomized controlled trial with 151 patients during 2012-2014. Costs of the intervention were estimated with a health sector perspective following international guidelines for CU. Quality of life was assessed using the 36-Item Short Form Health Survey.
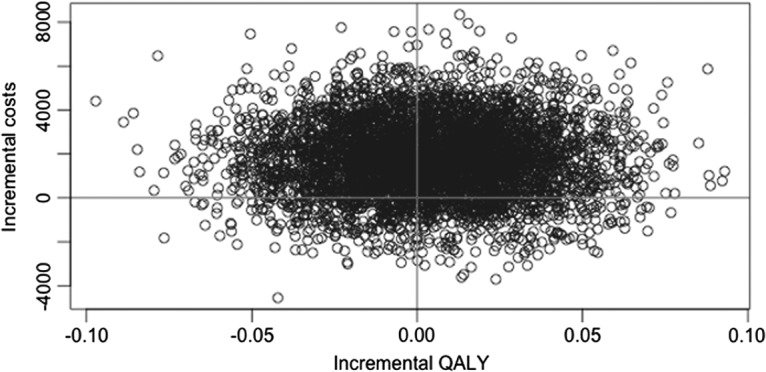
Results: The rehabilitation activities were approximately the same in the two groups, but the number of contacts with the physiotherapist was higher among the intervention group. The mean total cost per patient was €1,700 higher in the intervention group. The quality-adjusted life-years (QALYs) gain was higher in the intervention group, but the difference was not statistically significant. The incremental CU ratio was more than €400,000 per QALY gained.
Conclusions: Even though the rehabilitation activities increased, the program does not appear to be cost-effective. The intervention itself was not costly (less than €500), and increasing the number of patients may show reduced costs of the devices and make the CTR more cost-effective. Telerehabilitation can increase participation, but the intervention, in its current form, does not appear to be cost-effective.
Trial registration: ClinicalTrials.gov NCT01752192.
Keywords: cost-utility; economic evaluation; heart patients; randomized study; telerehabilitation.
Figures
References
-
- Economist Intelligence Unit. The heart of the matter: Rethinking prevention of cardiovascular disease. Available at www.economistinsights.com/healthcare/analysis/heartmatter (last accessed July5, 2015)
-
- Jolliffe JA, Rees K, Taylor RS, et al. Exercise-based rehabilitation for coronary heart diseases. Cochrane Database Syst Rev 2001;(1):CD001800. - PubMed
-
- Bjarnason-Wehrens B. Results from the European Cardiac Rehablitation Intventory Survey (ECRIS). European Association for Cardiovascular Prevention and Rehabilitation 2008. Eur J Cardiovasc Prev Rehabil 2010;17:410–418 - PubMed
-
- Meyer J. Meeting the challenges facing low cardic rehabilitation referral and participation rates. Circulation 2012;125:1321–1329 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
