

10-y Risks of Death and Emergency Re-admission in Adolescents Hospitalised with Violent, Drug- or Alcohol-Related, or Self-Inflicted Injury: A Population-Based Cohort Study
- PMID: 26714280
- PMCID: PMC4699823
- DOI: 10.1371/journal.pmed.1001931
10-y Risks of Death and Emergency Re-admission in Adolescents Hospitalised with Violent, Drug- or Alcohol-Related, or Self-Inflicted Injury: A Population-Based Cohort Study
Abstract
Background: Hospitalisation for adversity-related injury (violent, drug/alcohol-related, or self-inflicted injury) has been described as a "teachable moment", when intervention may reduce risks of further harm. Which adolescents are likely to benefit most from intervention strongly depends on their long-term risks of harm. We compared 10-y risks of mortality and re-admission after adversity-related injury with risks after accident-related injury.
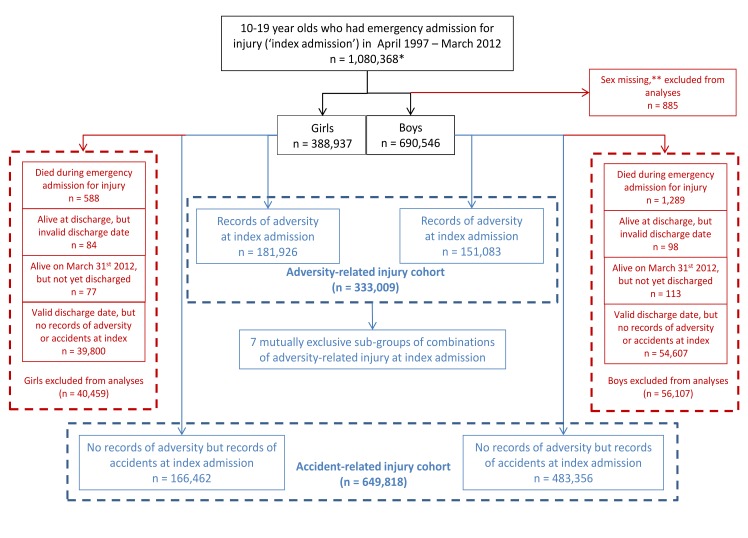
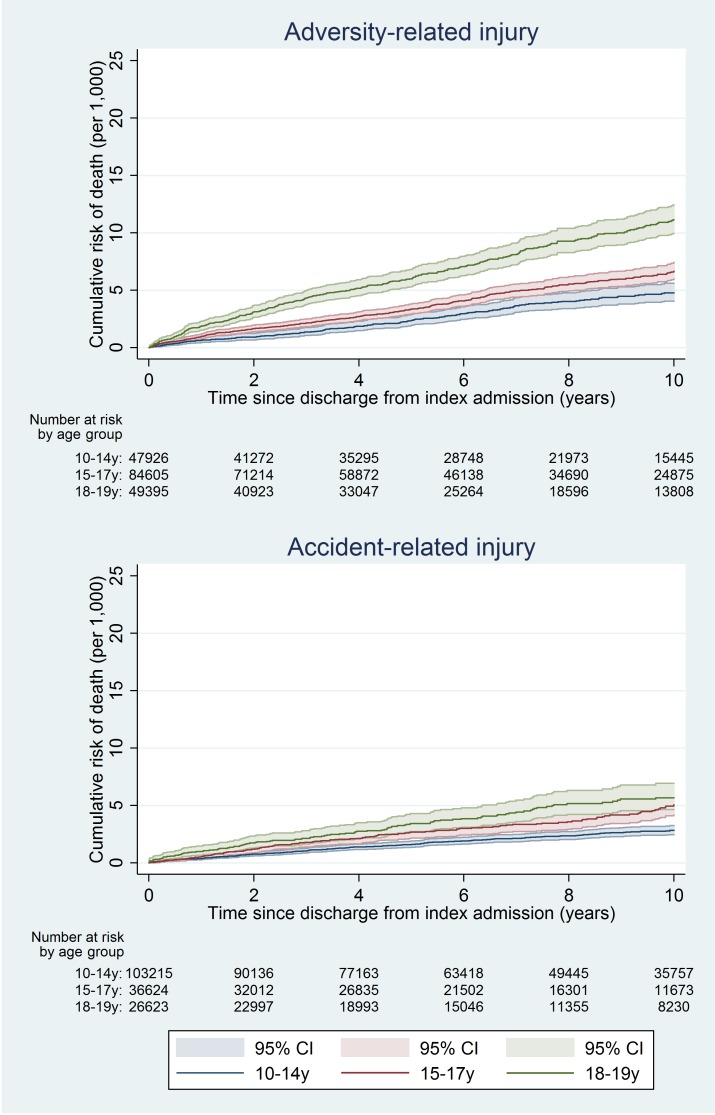
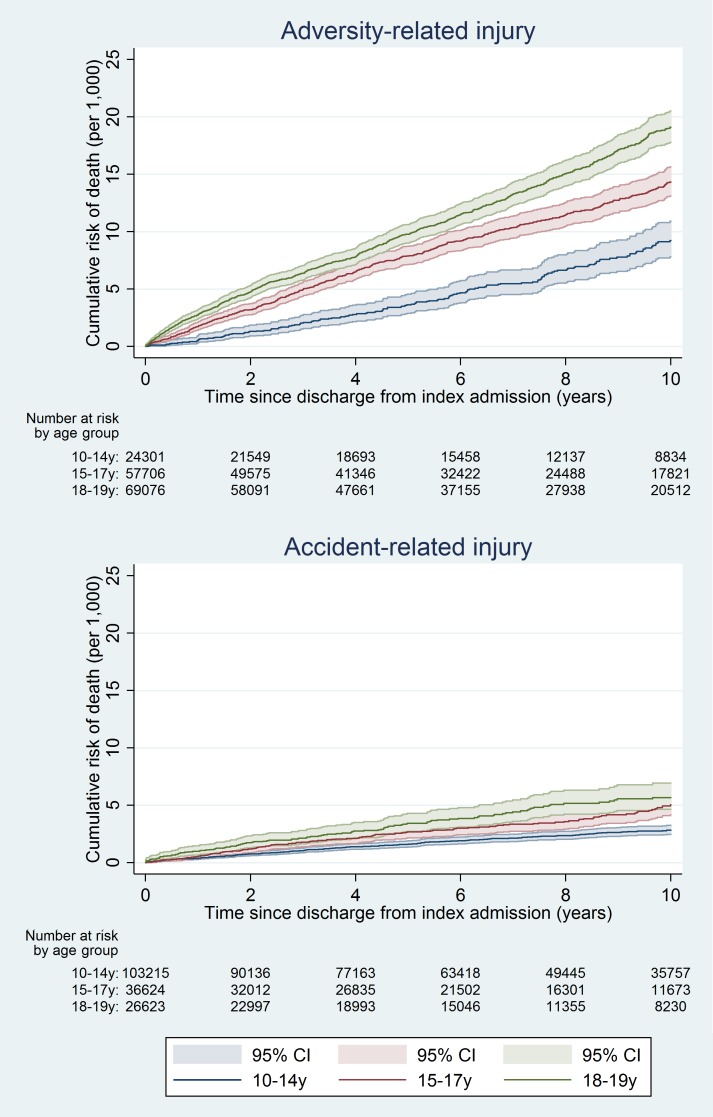
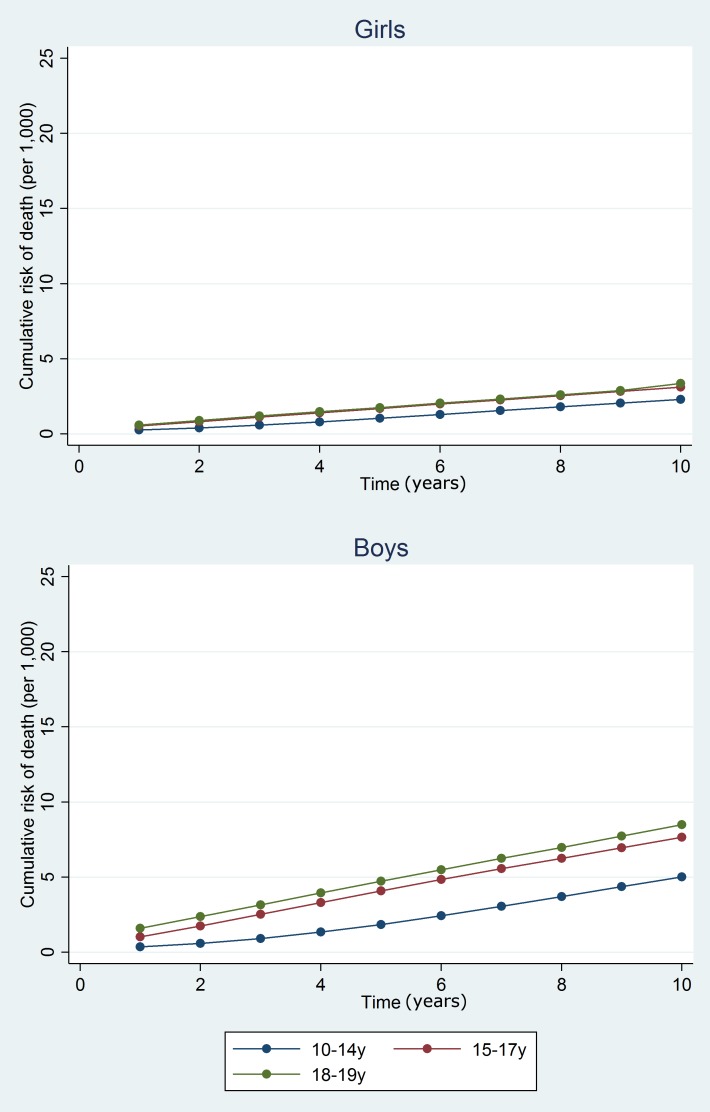
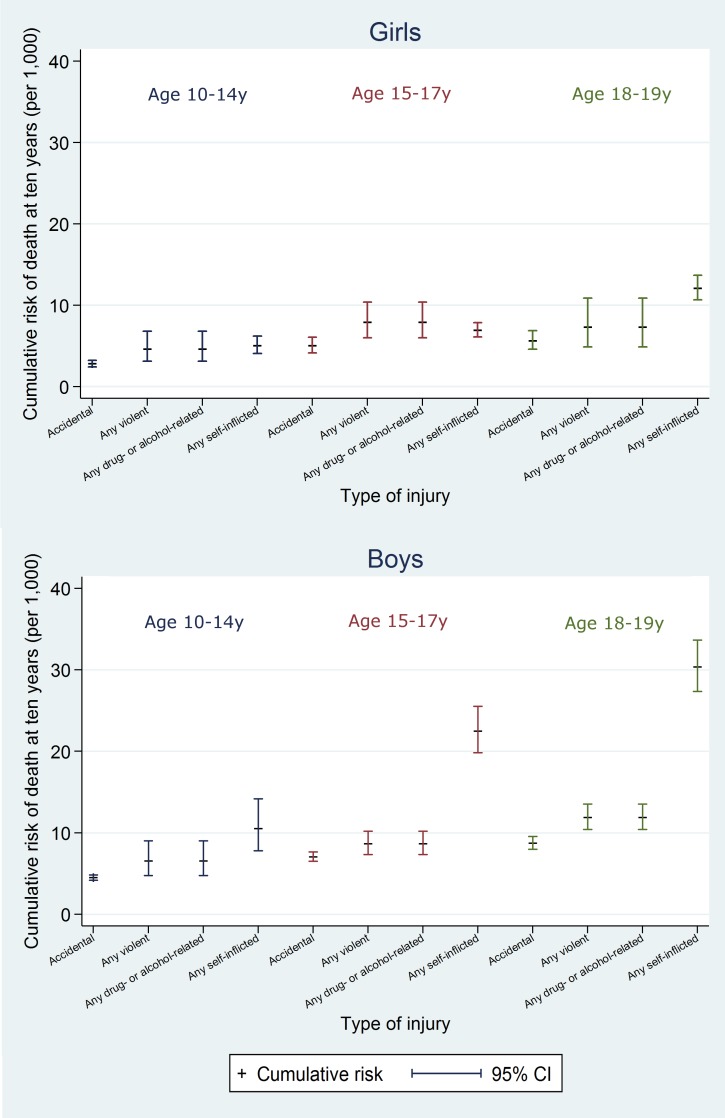
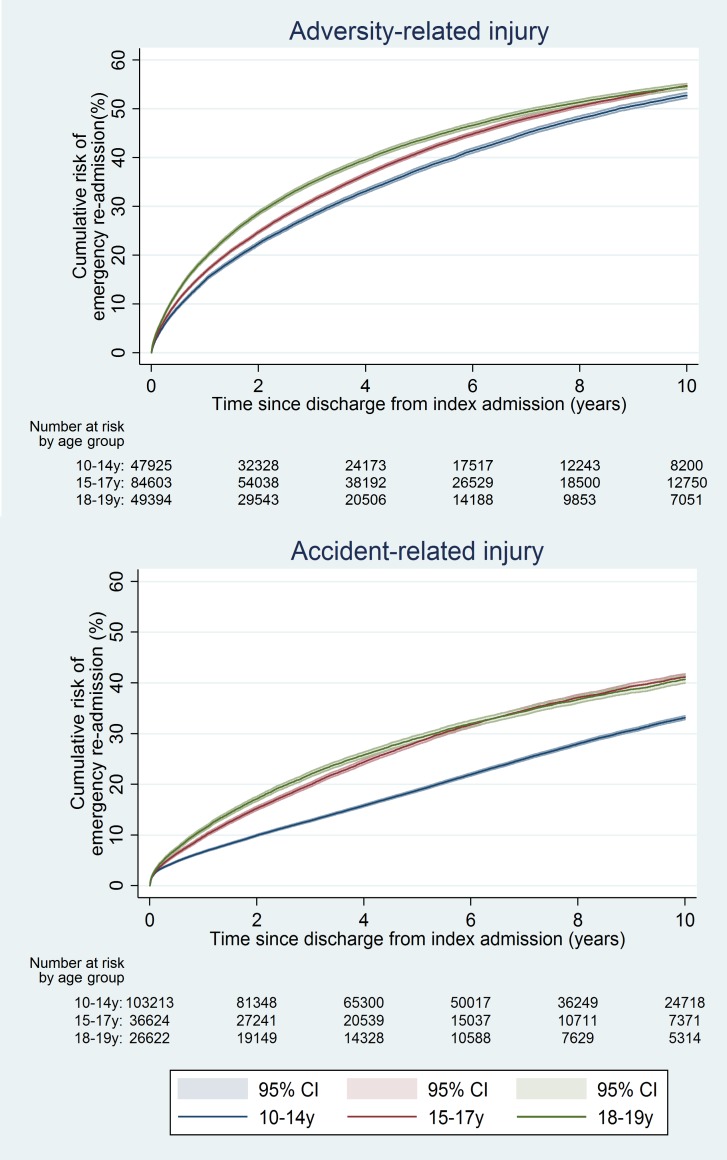
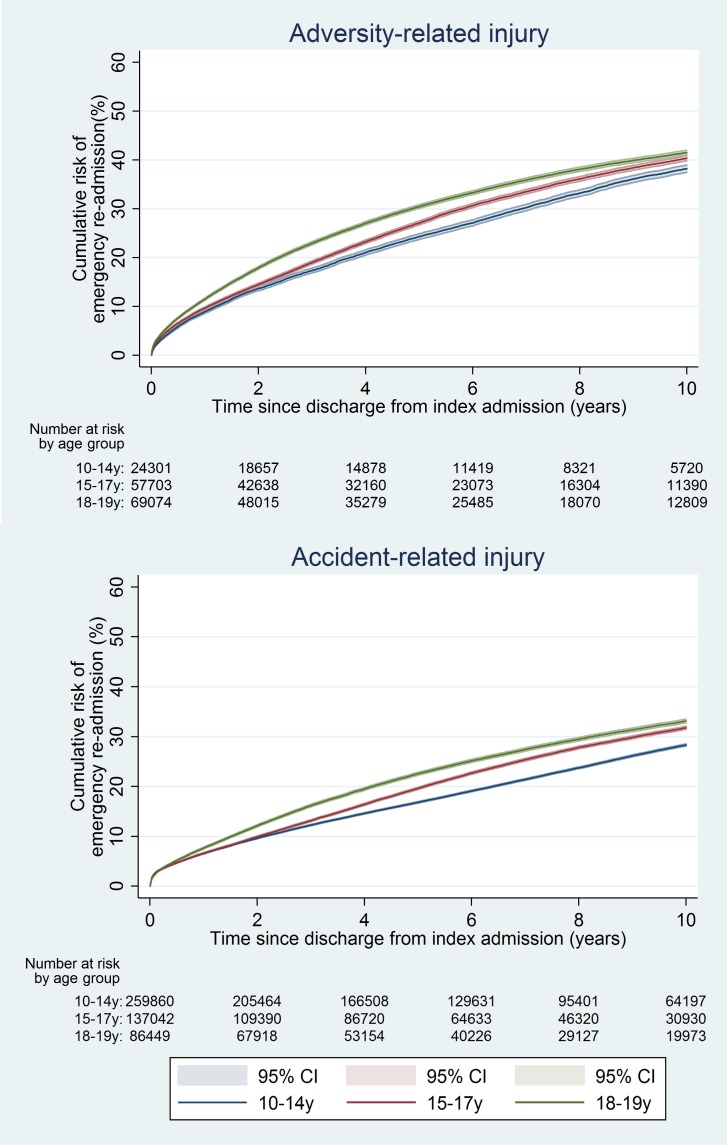
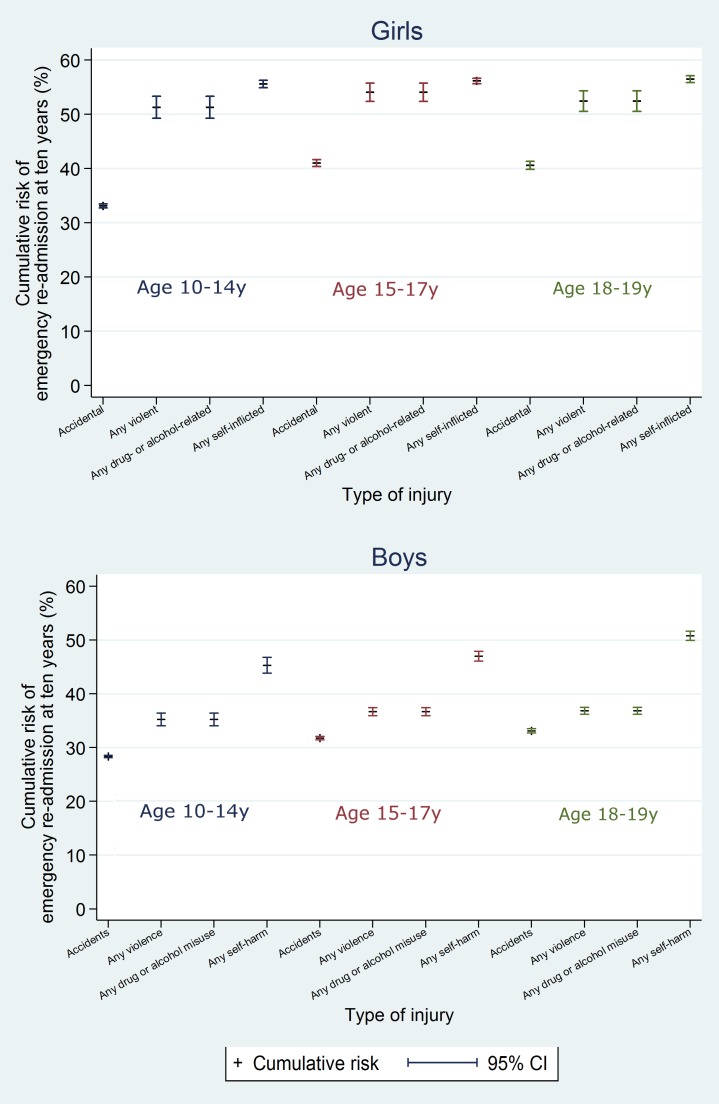
Methods and findings: We analysed National Health Service admissions data for England (1 April 1997-31 March 2012) for 10-19 y olds with emergency admissions for adversity-related injury (violent, drug/alcohol-related, or self-inflicted injury; n = 333,009) or for accident-related injury (n = 649,818). We used Kaplan-Meier estimates and Cox regression to estimate and compare 10-y post-discharge risks of death and emergency re-admission. Among adolescents discharged after adversity-related injury, one in 137 girls and one in 64 boys died within 10 y, and 54.2% of girls and 40.5% of boys had an emergency re-admission, with rates being highest for 18-19 y olds. Risks of death were higher than in adolescents discharged after accident-related injury (girls: age-adjusted hazard ratio 1.61, 95% CI 1.43-1.82; boys: 2.13, 95% CI 1.98-2.29), as were risks of re-admission (girls: 1.76, 95% CI 1.74-1.79; boys: 1.41, 95% CI 1.39-1.43). Risks of death and re-admission were increased after all combinations of violent, drug/alcohol-related, and self-inflicted injury, but particularly after any drug/alcohol-related or self-inflicted injury (i.e., with/without violent injury), for which age-adjusted hazard ratios for death in boys ranged from 1.67 to 5.35, compared with 1.25 following violent injury alone (girls: 1.09 to 3.25, compared with 1.27). The main limitation of the study was under-recording of adversity-related injuries and misclassification of these cases as accident-related injuries. This misclassification would attenuate the relative risks of death and re-admission for adversity-related compared with accident-related injury.
Conclusions: Adolescents discharged after an admission for violent, drug/alcohol-related, or self-inflicted injury have increased risks of subsequent harm up to a decade later. Introduction of preventive strategies for reducing subsequent harm after admission should be considered for all types of adversity-related injury, particularly for older adolescents.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Adolescents with adversity related injury are more at risk of death than those with accidental injuries, finds study.BMJ. 2015 Dec 30;351:h6986. doi: 10.1136/bmj.h6986. BMJ. 2015. PMID: 26721258 No abstract available.
References
-
- Currie C, Zanotti C, Morgan A, Currie D, de Looze M, et al. (2012) Social determinants of health and well-being among young people Health Behaviour in School-Aged Children (HBSC) study: international report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe.
-
- Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, et al. (2012) The 2011 ESPAD report: substance use among students in 36 European countries Stockholm: Swedish Council for Information on Alcohol and Other Drugs.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
