

Serum potassium levels, cardiac arrhythmias, and mortality following non-ST-elevation myocardial infarction or unstable angina: insights from MERLIN-TIMI 36
- PMID: 26714972
- PMCID: PMC5410890
- DOI: 10.1177/2048872615624241
Serum potassium levels, cardiac arrhythmias, and mortality following non-ST-elevation myocardial infarction or unstable angina: insights from MERLIN-TIMI 36
Abstract
Background: In acute coronary syndrome (ACS), potassium levels <3.5 mEq/L are associated with ventricular arrhythmias. Current guidelines therefore recommend a potassium target >4.0 mEq/L in ACS. Our study evaluated the association between potassium levels, cardiac arrhythmias, and cardiovascular death in patients with non-ST-segment elevation myocardial infarction or unstable angina.
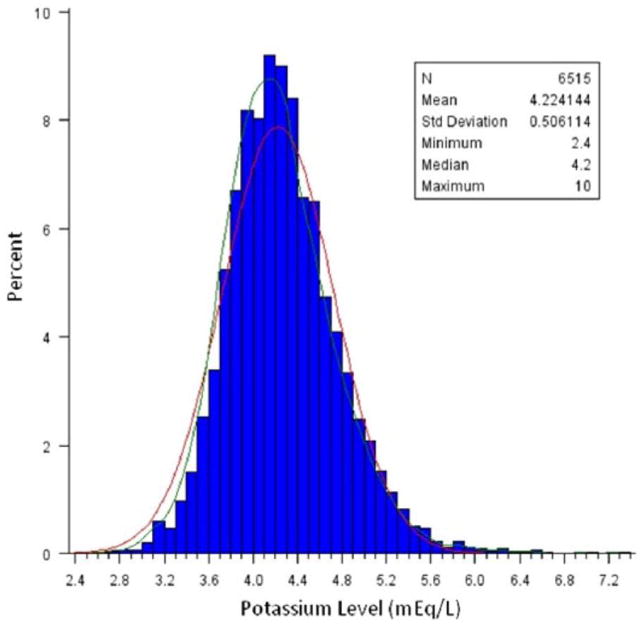
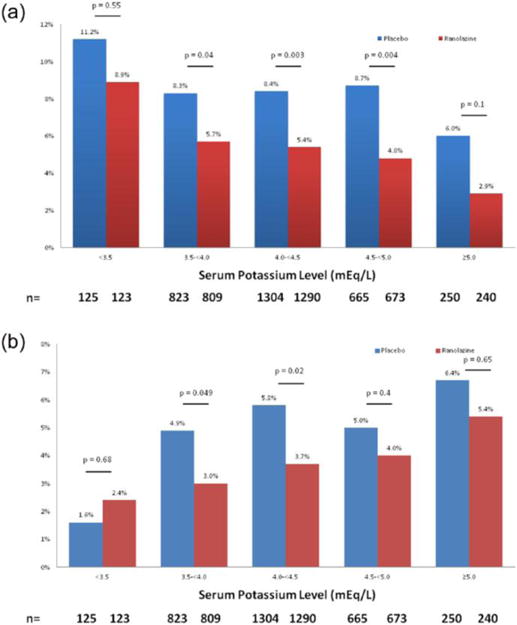
Methods: Potassium levels were measured in 6515 patients prior to randomization to receive either ranolazine or a placebo in the MERLIN-TIMI 36 trial. A seven-day continuous electrocardiographic assessment was obtained to determine the incidence of non-sustained ventricular tachycardia (NSVT) and ventricular pauses. The association between potassium levels and cardiovascular death was evaluated using a Cox proportional hazards regression model with multivariable adjustment.
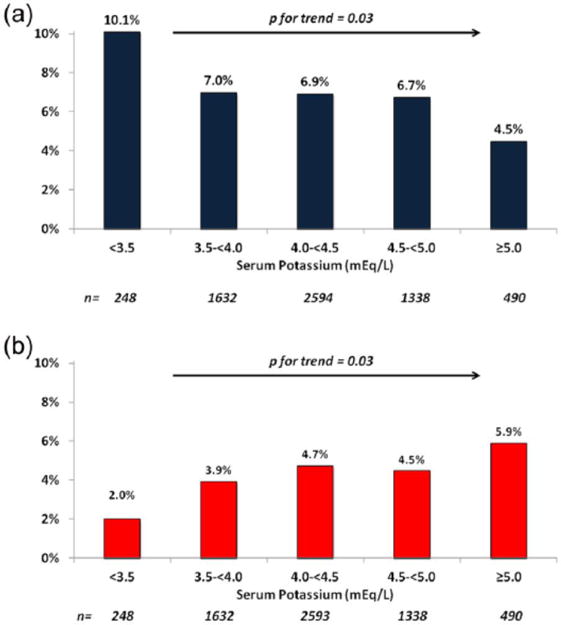
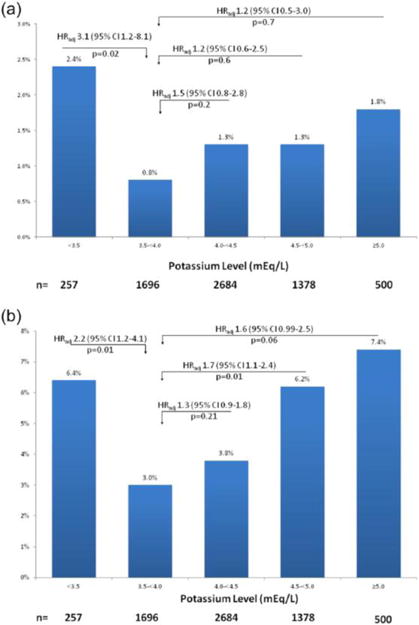
Results: NSVT lasting for at least eight consecutive beats occurred more frequently at potassium levels <3.5 mEq/L than at potassium levels ⩾5 mEq/L (10.1 vs. 4.5%, p=0.03 for trend), whereas the inverse pattern was observed for ventricular pauses >3 s, which occurred more frequently at potassium levels ⩾5 mEq/L than at potassium levels <3.5 mEq/L (5.9 vs. 2.0%, p=0.03 for trend). There was a U-shaped relationship between the potassium level at admission and both early and late risk of cardiovascular death. Compared with patients with potassium levels of 3.5 to <4 mEq/L, a potassium level <3.5 mEq/L was associated with an increased risk of cardiovascular death at day 14 (2.4 vs. 0.8%, HRadj 3.1, p=0.02) and at one year (6.4 vs. 3.0%, HRadj 2.2, p=0.01). The risk of cardiovascular death at one year was also significantly increased at potassium levels ⩾4.5 mEq/L and a similar trend was noted at potassium levels ⩾5 mEq/L.
Conclusions: The lowest risk of cardiovascular death was observed in patients with admission potassium levels between 3.5 and 4.5 mEq/L. Both lower and higher levels of potassium were associated with tachyarrhythmias and bradyarrhythmias, suggesting a potential mechanistic explanation for the increased risk of cardiovascular death at the extremes of potassium homeostasis.
Keywords: Arrhythmias; acute coronary syndrome; cardiovascular death; myocardial infarction; potassium levels; ventricular tachycardia.
Conflict of interest statement
Ravi B Patel, Sara Tannenbaum, Ana Viana-Tejedor, Jianping Guo, and KyungAh Im have nothing to disclose.
Benjamin M Scirica reports grants from Gilead, during the conduct of the study; grants from AstraZeneca, grants from Bristol-Myers Squibb, grants from Daichi-Sankyo, grants from Johnson and Johnson, grants from Bayer Healthcare, grants from Gilead, grants from Eisai, grants from Merck, personal fees from Gilead, personal fees from Lexicon, personal fees from Arena, personal fees from Eisai, personal fees from St Jude’s Medical, personal fees from Boston Clinical Research Institute, fees from University of Calgary, personal fees from Elsevier Practice Update Cardiology, personal fees from Forest Pharmaceuticals, personal fees from Boehringer Ingelheim, personal fees from Merck, personal fees from GlaxoSmithKline, personal fees from GE Healthcare, and personal fees from BiogenIdec, outside the submitted work.
Figures
References
-
- Grumbach L, Howard JW, Merrill VI. Factors related to the initiation of ventricular fibrillation in the isolated heart; effect of calcium and potassium. Circ Res. 1954;2:452–459. - PubMed
-
- Brown MJ, Brown DC, Murphy MB. Hypokalemia from beta2-receptor stimulation by circulating epinephrine. N Engl J Med. 1983;309:1414–1419. - PubMed
-
- Hulting J. In-hospital ventricular fibrillation and its relation to serum potassium. Acta Med Scand Suppl. 1981;647:109–116. - PubMed
-
- Kafka H, Langevin L, Armstrong PW. Serum magnesium and potassium in acute myocardial infarction. Influence on ventricular arrhythmias Arch Intern Med. 1987;147:465–469. - PubMed
-
- Solomon RJ, Cole AG. Importance of potassium in patients with acute myocardial infarction. Acta Med Scand Suppl. 1981;647:87–93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
