

MRI for the preoperative evaluation of femoroacetabular impingement
- PMID: 26715128
- PMCID: PMC4805622
- DOI: 10.1007/s13244-015-0459-0
MRI for the preoperative evaluation of femoroacetabular impingement
Abstract
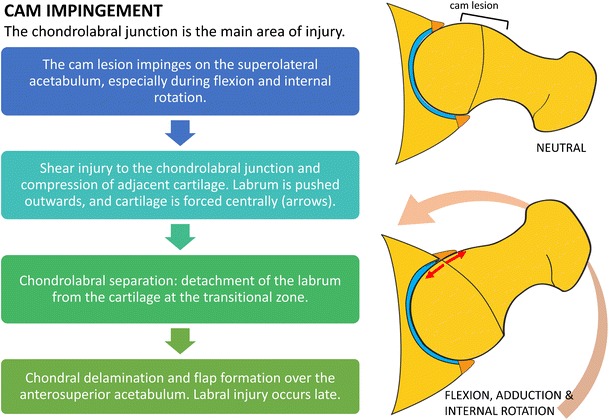
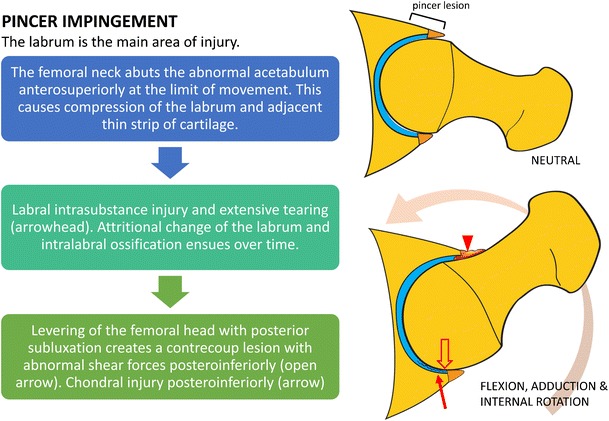
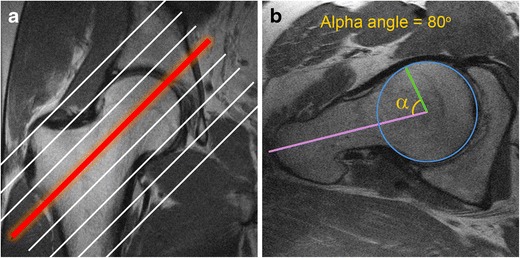
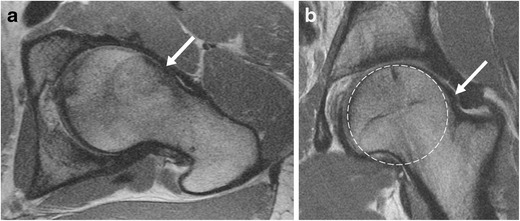
Femoroacetabular impingement (FAI) refers to a condition characterized by impingement of the femoral head-neck junction against the acetabular rim, often due to underlying osseous and/or soft tissue morphological abnormalities. It is a common cause of hip pain and limited range of motion in young and middle-aged adults. Hip preservation surgery aims to correct the morphological variants seen in FAI, thereby relieving pain and improving function, and potentially preventing early osteoarthritis. The purpose of this article is to review the mechanisms of chondral and labral injury in FAI to facilitate an understanding of patterns of chondrolabral injury seen on MRI. Preoperative MRI evaluation of FAI should include assessment of osseous morphologic abnormalities, labral tears, cartilage status, and other associated compensatory injuries of the pelvis. As advanced chondral wear is the major relative contraindication for hip preservation surgery, MRI is useful in the selection of patients likely to benefit from surgery. Teaching points • The most common anatomical osseous abnormalities predisposing to FAI include cam and pincer lesions. • Morphological abnormalities, labral lesions, and cartilage status should be assessed. • In cam impingement, chondral wear most commonly occurs anterosuperiorly.• Pre-existing advanced osteoarthritis is the strongest predictor of poor outcomes after FAI surgery. • Injury to muscles and tendons or other pelvic structures can coexist with FAI.
Keywords: Arthroscopy; Cartilage; Femoroacetabular impingement; Magnetic resonance imaging; Preoperative.
Figures
References
-
- Nawabi DH, Bedi A, Tibor LM, Magennis E, Kelly BT. The demographic characteristics of high-level and recreational athletes undergoing hip arthroscopy for femoroacetabular impingement: a sports-specific analysis. Arthroscopy: J Arthroscopic Related Surg: Off Publ Arthroscopy Assoc North Am Int Arthroscopy Assoc. 2014;30(3):398–405. doi: 10.1016/j.arthro.2013.12.010. - DOI - PubMed
-
- Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
