

Acute kidney injury treated with renal replacement therapy and 5-year mortality after myocardial infarction-related cardiogenic shock: a nationwide population-based cohort study
- PMID: 26715162
- PMCID: PMC4699352
- DOI: 10.1186/s13054-015-1170-8
Acute kidney injury treated with renal replacement therapy and 5-year mortality after myocardial infarction-related cardiogenic shock: a nationwide population-based cohort study
Abstract
Background: Myocardial infarction-related cardiogenic shock is frequently complicated by acute kidney injury. We examined the influence of acute kidney injury treated with renal replacement therapy (AKI-RRT) on risk of chronic dialysis and mortality, and assessed the role of comorbidity in patients with cardiogenic shock.
Methods: In this Danish cohort study conducted during 2005-2012, we used population-based medical registries to identify patients diagnosed with first-time myocardial infarction-related cardiogenic shock and assessed their AKI-RRT status. We computed the in-hospital mortality risk and adjusted relative risk. For hospital survivors, we computed 5-year cumulative risk of chronic dialysis accounting for competing risk of death. Mortality after discharge was computed with use of Kaplan-Meier methods. We computed 5-year hazard ratios for chronic dialysis and death after discharge, comparing AKI-RRT with non-AKI-RRT patients using a propensity score-adjusted Cox regression model.
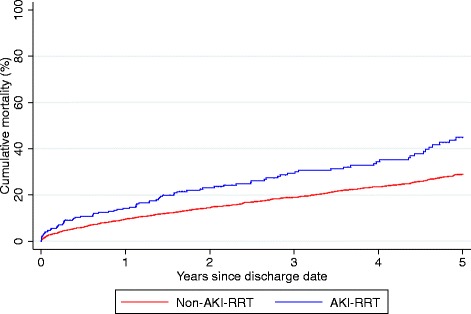
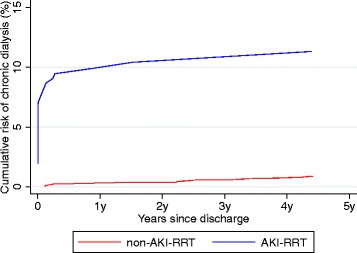
Results: We identified 5079 patients with cardiogenic shock, among whom 13% had AKI-RRT. The in-hospital mortality was 62% for AKI-RRT patients, and 36% for non-AKI-RRT patients. AKI-RRT remained associated with increased in-hospital mortality after adjustment for confounders (relative risk=1.70, 95% confidence interval (CI): 1.59-1.81). Among the 3059 hospital survivors, the 5-year risk of chronic dialysis was 11% (95% CI: 8-16%) for AKI-RRT patients, and 1% (95% CI: 0.5-1%) for non-AKI-RRT patients (adjusted hazard ratio: 15.9 (95% CI: 8.7-29.3). The 5-year mortality was 43% (95% CI: 37-53%) for AKI-RRT patients compared with 29% (95% CI: 29-31%) for non-AKI-RRT patients. The adjusted 5-year hazard ratio for death was 1.55 (95% CI: 1.22-1.96) for AKI-RRT patients compared with non-AKI-RRT patients. In patients with comorbidity, absolute mortality increased while relative impact of AKI-RRT on mortality decreased.
Conclusion: AKI-RRT following myocardial infarction-related cardiogenic shock predicted elevated short-term mortality and long-term risk of chronic dialysis and mortality. The impact of AKI-RRT declined with increasing comorbidity suggesting that intensive treatment of AKI-RRT should be accompanied with optimized treatment of comorbidity when possible.
Figures
References
-
- Schmidt M, Jacobsen JB, Lash TL, Botker HE, Sorensen HT. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344 doi: 10.1136/bmj.e356. - DOI - PMC - PubMed
-
- Dubey L, Sharma S, Gautam M, Gautam S, Guruprasad S, Subramanyam G. Cardiogenic shock complicating acute myocardial infarction—a review. Acta Cardiol. 2011;66(6):691–9. - PubMed
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119(9):1211–9. doi: 10.1161/CIRCULATIONAHA.108.814947. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
