

Impact of country-specific EQ-5D-3L tariffs on the economic value of systemic therapies used in the treatment of metastatic pancreatic cancer
- PMID: 26715881
- PMCID: PMC4687669
- DOI: 10.3747/co.22.2592
Impact of country-specific EQ-5D-3L tariffs on the economic value of systemic therapies used in the treatment of metastatic pancreatic cancer
Abstract
Background: Previous Canadian cost-effectiveness analyses in cancer based on the EQ-5D-3L (EuroQoL, Rotterdam, Netherlands) have commonly used U.K. or U.S. tariffs because the Canadian equivalent only just recently became available. The implications of using non-Canadian tariffs to inform decision-making are unclear. We aimed to reevaluate an earlier cost-effectiveness analysis of therapies for metastatic pancreatic cancer (originally performed using U.S. tariffs) with tariffs from Canada and various other countries to determine the impact of using non-country-specific tariffs.
Methods: We used tariffs from Canada, the United States, the United Kingdom, Denmark, France, Germany, Japan, the Netherlands, and Spain to derive EQ-5D-3L utilities for the 10 health states in the pancreatic cancer model. Quality-adjusted life years (qalys) and incremental cost-effectiveness ratios (icers) were generated, and probabilistic sensitivity analyses (psas) were performed.
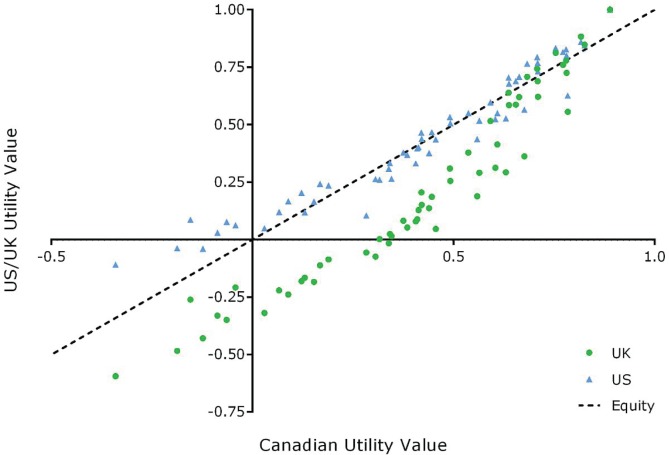
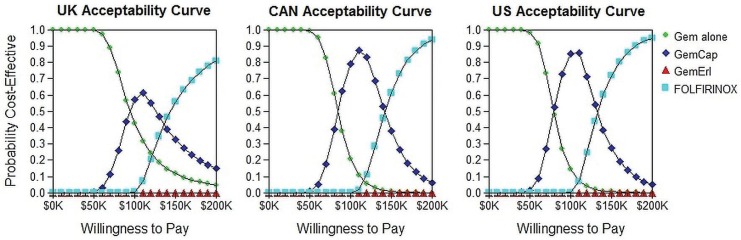
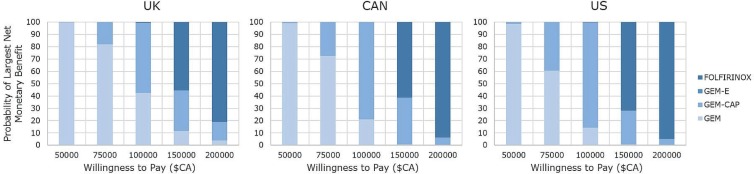
Results: Canadian utilities are generally lower than the corresponding U.S. utilities and higher than those for the United Kingdom. Compared with the Canadian-valued scenarios, U.S. and U.K. estimates were statistically different for 3 and 9 scenarios respectively. Overall, 35% of the non-Canadian utilities (28 of 80) were significantly different, clinically, from the Canadian values. Canadian qalys were 6% lower than those for the United States and 6% higher than those for the United Kingdom. When comparing the qalys of each treatment with those of gemcitabine alone, the average percent change was +6.8% for a U.S. scenario and -7.5% for a U.K. scenario compared with a Canadian scenario. Consequently, Canadian icers were approximately 5.4% greater than those for the United States and 8.6% lower than those for the United Kingdom. Based on the psas and compared with the Canadian threshold value, the minimum willingness-to-pay threshold at which the combination chemotherapy regimen of gemcitabine-capecitabine is the most cost-effective is $5,239 less than in the United States and $11,986 more than in the United Kingdom.
Conclusions: The use of non-country-specific tariffs leads to significant differences in the derived utilities, icers, and psa results. Past Canadian EQ-5D-3L-based cost-effectiveness analyses and related funding decisions might need to be re-visited using Canadian tariffs.
Keywords: EQ-5D-3L; Pancreatic cancer; cost-effectiveness; country-specific tariffs; weights.
Figures
References
-
- National Institute for Health and Care Excellence (nice) Social Value Judgements: Principles for the Development of NICE Guidance. 2nd ed. London, UK: NICE; 2008. - PubMed
-
- Canadian Agency for Drugs and Technologies in Health (cadth) Guidelines for the Economic Evaluation of Health Technologies: Canada. 3rd ed. Ottawa, ON: CADTH; 2006.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
