

Characteristics affecting survival after locally advanced colorectal cancer in Quebec
- PMID: 26715887
- PMCID: PMC4687675
- DOI: 10.3747/co.22.2692
Characteristics affecting survival after locally advanced colorectal cancer in Quebec
Abstract
Background: We estimated the relations of sociodemographic, organizational, disease, and treatment variables with the risk of death from colorectal cancer (crc) in a Quebec population-based sample of patients with locally advanced crc (lacrc) who underwent tumour resection with curative intent.
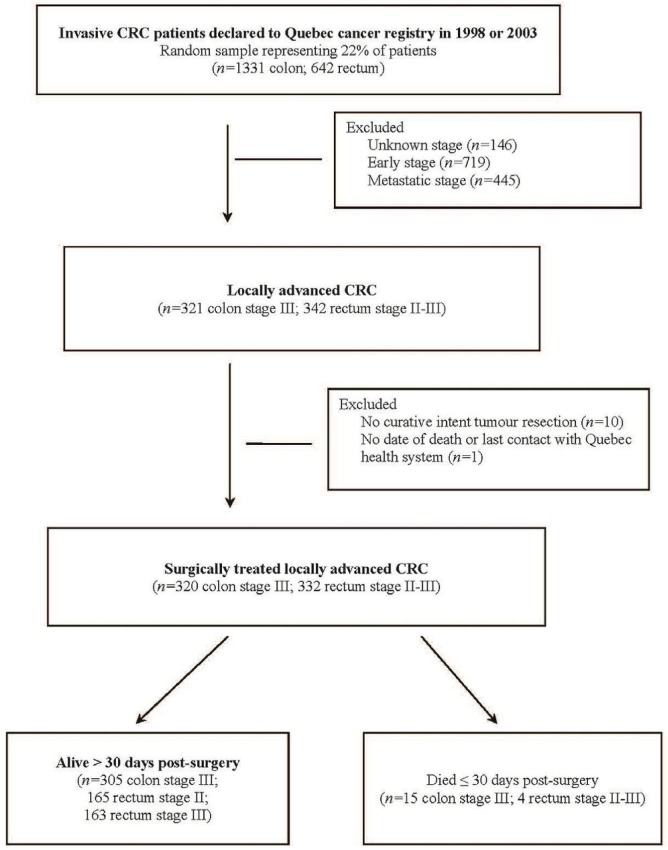
Methods: Information from medical records and administrative databases was obtained for a random sample of 633 patients surgically treated for stages ii-iii rectal and stage iii colon cancer and declared to the Quebec cancer registry in 1998 and 2003. We measured personal, disease, and clinical management characteristics, relative survival, and through multivariate modelling, relative excess rate (rer) of death.
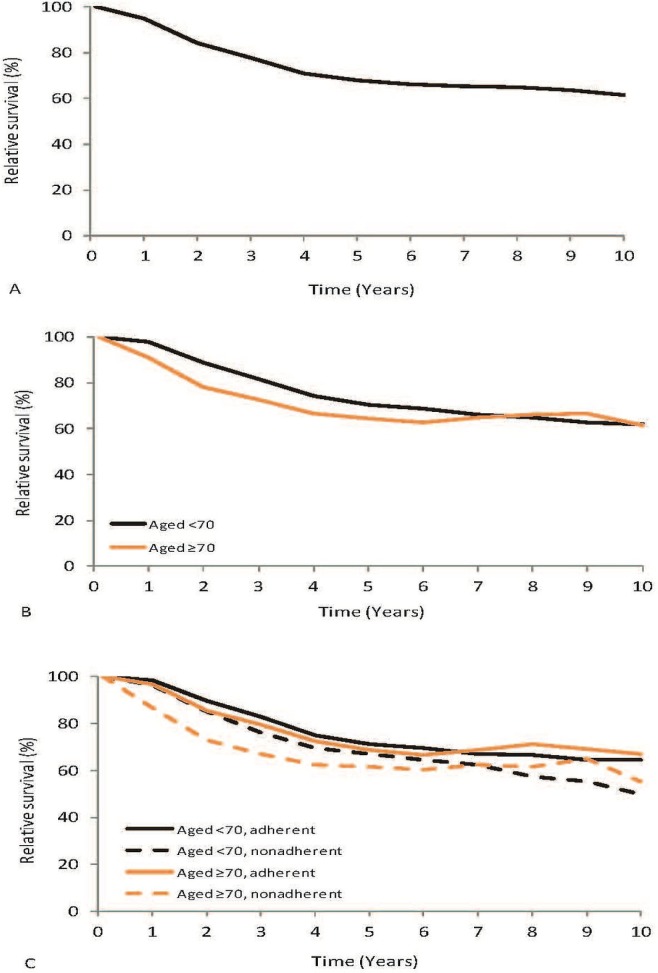
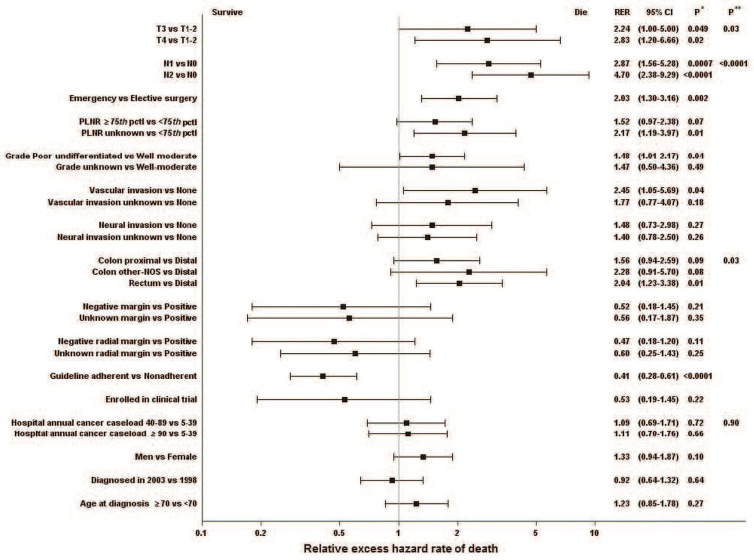
Results: The relative 5- and 10-year survivals in this cohort were 67.7% [95% confidence interval (ci): 65.8% to 69.6%] and 61.2% (95% ci: 58.3% to 64.0%) respectively. Stage T4, stage N2, and emergency rather than elective surgery affected 18%, 24% and 10% of patients respectively. Those disease progression characteristics each independently increased the rer of death by factors of 2 to almost 5. Grade, vascular invasion, and tumour location were also significantly associated with the rer for death. Receiving guideline-adherent treatment was associated with a 60% reduction in the rer for death (0.41; 95% ci: 0.28 to 0.61), an effect that was consistent across age groups. Clear margins (proximal-distal, radial) and clinical trial enrolment were each associated with a nonsignificant 50% reduction in the rer. Of patients less than 70 years of age and 70 years of age and older, 81.3% and 42.0% respectively received guideline-adherent treatment.
Conclusions: This study is the first Quebec population-based examination of patients with lacrc and their management, outcomes, and outcome determinants. The results can help in planning crc control strategies at a population level.
Keywords: Colorectal neoplasms; medical records; multivariate analyses; population-based studies; registries; relative excess hazard rate for death; relative survival; treatment outcomes.
Figures
Similar articles
-
Aspects of survival from colorectal cancer in Denmark.Dan Med J. 2012 Apr;59(4):B4428. Dan Med J. 2012. PMID: 22459726
-
Population-based assessment of the surgical management of locally advanced colorectal cancer.J Natl Cancer Inst. 2006 Oct 18;98(20):1474-81. doi: 10.1093/jnci/djj396. J Natl Cancer Inst. 2006. PMID: 17047196
-
Trends in Overall Survival and Treatment Patterns in Two Large Population-Based Cohorts of Patients with Breast and Colorectal Cancer.Cancers (Basel). 2019 Aug 23;11(9):1239. doi: 10.3390/cancers11091239. Cancers (Basel). 2019. PMID: 31450842 Free PMC article.
-
Comparable survival for young rectal cancer patients, despite unfavourable morphology and more advanced-stage disease.Eur J Cancer. 2015 Sep;51(13):1675-82. doi: 10.1016/j.ejca.2015.06.005. Epub 2015 Jul 6. Eur J Cancer. 2015. PMID: 26159248
-
Surgical approach in locally advanced colorectal cancer--combined, extended and compound surgery.Khirurgiia (Sofiia). 2013;(4):29-50. Khirurgiia (Sofiia). 2013. PMID: 24800318 Review. Bulgarian, English.
Cited by
-
Colorectal cancer survival among Malaysia population: data from the Malaysian National Cancer Registry.Front Oncol. 2023 Nov 29;13:1132417. doi: 10.3389/fonc.2023.1132417. eCollection 2023. Front Oncol. 2023. PMID: 38094603 Free PMC article.
-
Polo-like kinase 2 promotes chemoresistance and predicts limited survival benefit from adjuvant chemotherapy in colorectal cancer.Int J Oncol. 2018 May;52(5):1401-1414. doi: 10.3892/ijo.2018.4328. Epub 2018 Mar 20. Int J Oncol. 2018. PMID: 29568868 Free PMC article.
-
Contribution of Matrix Metalloproteinase-1 Genotypes to Colorectal Cancer in Taiwan.Cancer Genomics Proteomics. 2021 May-Jun;18(3):245-251. doi: 10.21873/cgp.20255. Epub 2021 Apr 23. Cancer Genomics Proteomics. 2021. PMID: 33893077 Free PMC article.
-
Effects of oxaliplatin-containing adjuvant chemotherapy on short-term survival of patients with colon cancer in Dr. Sardjito Hospital, Yogyakarta, Indonesia.J Gastrointest Oncol. 2019 Apr;10(2):226-234. doi: 10.21037/jgo.2018.12.10. J Gastrointest Oncol. 2019. PMID: 31032089 Free PMC article.
-
The Risk Factors Affecting Survival in Colorectal Cancer in Taiwan.Iran J Public Health. 2018 Apr;47(4):519-530. Iran J Public Health. 2018. PMID: 29900136 Free PMC article.
References
-
- Canadian Cancer Society’s Advisory Committee on Cancer Statistics . Canadian Cancer Statistics 2014. Toronto, ON: Canadian Cancer Society; 2014.
-
- Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German cao/aro/aio-94 randomized phase iii trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926–33. doi: 10.1200/JCO.2011.40.1836. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
